Evaluation of Ultra-Low Dose CT in the Diagnosis of Pediatric-Like Fractures Using an Experimental Animal Study
- Affiliations
-
- 1Department of Diagnostic Radiology, Pediatric Radiology and Sonography, University Hospital Schleswig-Holstein, Campus Kiel, 24105 Kiel, Germany. joerg.d.moritz@rad.uni-kiel.de
- 2Department of Diagnostic Radiology, University Hospital Schleswig-Holstein, Campus Kiel, 24105 Kiel, Germany.
- 3Department of Medical Informatics and Statistics, University Hospital Schleswig-Holstein, Campus Kiel, 24105 Kiel, Germany.
- 4North German Seminar of Radiation Protection, University Kiel, 24098 Kiel, Germany.
- KMID: 1245380
- DOI: http://doi.org/10.3348/kjr.2012.13.2.165
Abstract
OBJECTIVE
The aim of this prospective study was to evaluate the performance of ultra-low dose CT for the diagnosis of pediatric-like fractures and ascertain the lowest dose level sufficient for diagnostics.
MATERIALS AND METHODS
Fifty-one bones of young pig cadavers were artificially fractured and subsequently examined by using a 64 multi-detector CT with 36 various dose levels down to a dose comparable with that of X-rays. Two pediatric radiologists analysed the CT scans according to the presence or absence of a fracture, determination of the fracture type and the displacement as well as the diagnostic certainty. For each dose protocol, a success rate for the correct determination of the above-mentioned CT analyses was calculated. A success rate of at least 95% was considered sufficient for diagnostics.
RESULTS
All but the lowest dose levels were sufficient to identify the fracture. Only the two lowest dose levels were insufficient to detect the fracture type. All dose levels were adequate for the identification of the displacement. The lowest dose level sufficient for diagnostics was 120 kVp, 11 mAs, and pitch 1.5, with a CTDIvol of 10% of a standard dose and an effective dose three times as large as that of X-rays.
CONCLUSION
Ultra-low dose CT provides the feasibility of a significant dose reduction, still allowing sufficient diagnostics of pediatric-like fractures.
MeSH Terms
Figure
-

Fig. 1 Longitudinal fracture with extension into epiphysial plate (Salter Harris II) of third metacarpal bone (black arrow). Oblique fracture with step of second metacarpal bone (white triangle). All dose levels were diagnostic. A. Reference protocol 120 kVp, 100 mAs, pitch 0.9. B. Routine standard protocol 120 kVp, 50 mAs, pitch 0.9. C. 50% of dose of standard protocol 120 kVp, 40 mAs, pitch 1.5. D. 30% of dose of standard protocol 120 kVp, 20 mAs, pitch 1.5. E. 10% of dose of standard protocol 120 kVp, 11 mAs, pitch 1.5. F. Lowest dose protocol of study 80 kVp, 11 mAs, pitch 1.5.
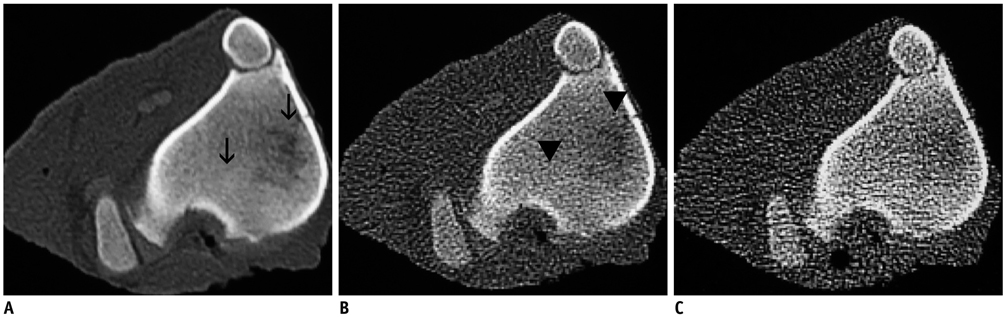
Fig. 2 Undislocated fissure of tibial head. Fracture is seen in high dose protocol (120 kVp, 100 mAs, pitch 0.9, A, black arrow) as well as in ultra-low dose protocol (120 kVp, 11 mAs, pitch 1.5, B, black triangles). Fracture is missed at lowest dose level (80 kVp, 11 mAs, pitch 1.5, C).

Fig. 3 Comminuted fractures of second and third metacarpals with step and impression (black arrow). All dose levels were diagnostic-A. 120 kVp, 100 mAs, pitch 0.9. B. 120 kVp, 11 mAs, pitch 1.5. C. 80 kVp, 11 mAs, pitch 1.5.
Reference
-
1. Cho KH, Lee SM, Lee YH, Suh KJ. Ultrasound diagnosis of either an occult or missed fracture of an extremity in pediatric-aged children. Korean J Radiol. 2010. 11:84–94.2. Moritz JD, Berthold LD, Soenksen SF, Alzen GF. Ultrasound in diagnosis of fractures in children: unnecessary harassment or useful addition to X-ray? Ultraschall Med. 2008. 29:267–274.3. Moritz JD, Hoffmann B, Meuser SH, Sehr DH, Caliebe A, Heller M. [Is ultrasound equal to X-ray in pediatric fracture diagnosis?]. Rofo. 2010. 182:706–771.4. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol. 2001. 176:289–296.5. Diederichs CG, Engelke WG, Richter B, Hermann KP, Oestmann JW. Must radiation dose for CT of the maxilla and mandible be higher than that for conventional panoramic radiography? AJNR Am J Neuroradiol. 1996. 17:1758–1760.6. Mulkens TH, Marchal P, Daineffe S, Salgado R, Bellinck P, te Rijdt B, et al. Comparison of low-dose with standard-dose multidetector CT in cervical spine trauma. AJNR Am J Neuroradiol. 2007. 28:1444–1450.7. Dammert S, Funke M, Merten HA, Obernauer S, Grabbe E. [Multislice helical CT (MSCT) for mid-facial trauma: Optimization of parameters for scanning and reconstruction]. Rofo. 2002. 174:874–879.8. Bohy P, de Maertelaer V, Roquigny A, Keyzer C, Tack D, Gevenois PA. Multidetector CT in patients suspected of having lumbar disk herniation: comparison of standard-dose and simulated low-dose techniques. Radiology. 2007. 244:524–531.9. Connor SE, Arscott T, Berry J, Greene L, O'Gorman R. Precision and accuracy of low-dose CT protocols in the evaluation of skull landmarks. Dentomaxillofac Radiol. 2007. 36:270–276.10. Lutz J, Jäger V, Hempel MJ, Srivastav S, Reiser M, Jäger L. Delineation of temporal bone anatomy: feasibility of low-dose 64-row CT in regard to image quality. Eur Radiol. 2007. 17:2638–2645.11. Chassang M, Grimaud A, Cucchi JM, Novellas S, Amoretti N, Chevallier P, et al. Can low-dose computed tomographic scan of the spine replace conventional radiography? An evaluation based on imaging myelomas, bone metastases, and fractures from osteoporosis. Clin Imaging. 2007. 31:225–222.12. Goodman LA. On simultaneous confidence intervals for multinominal proportions. Technometrics. 1965. 7:247–254.13. Stuart A. A test for homogeneity of the marginal distribution in a two way classification. Biometrika. 1955. 42:412–416.14. R Development Core Team. R: A language and environment for statistical computing. Version 2.10.1., 2009. R Foundation for Statistical Computing. 2007. Vienna, Austria: http://www.R-project.org. ISBN: 3-900-051-07-0.15. Horger M, Claussen CD, Bross-Bach U, Vonthein R, Trabold T, Heuschmid M, et al. Whole-body low-dose multidetector row-CT in the diagnosis of multiple myeloma: an alternative to conventional radiography. Eur J Radiol. 2005. 54:289–297.16. Gleeson TG, Moriarty J, Shortt CP, Gleeson JP, Fitzpatrick P, Byrne B, et al. Accuracy of whole-body low-dose multidetector CT (WBLDCT) versus skeletal survey in the detection of myelomatous lesions, and correlation of disease distribution with whole-body MRI (WBMRI). Skeletal Radiol. 2009. 38:225–236.17. Huda W, Vance A. Patient radiation doses from adult and pediatric CT. AJR Am J Roentgenol. 2007. 188:540–546.18. Kluner C, Hein PA, Gralla O, Hein E, Hamm B, Romano V, et al. Does ultra-low-dose CT with a radiation dose equivalent to that of KUB suffice to detect renal and ureteral calculi? J Comput Assist Tomogr. 2006. 30:44–50.19. Rogalla P, Klüner C, Taupitz M. [Ultra-low-dose CT to search for stones in kidneys and collecting system]. Aktuelle Urol. 2004. 35:307–309.20. Cohnen M, Vogt C, Beck A, Andersen K, Heinen W, vom Dahl S, et al. Feasibility of MDCT Colonography in ultra-low-dose technique in the detection of colorectal lesions: comparison with high-resolution video colonoscopy. AJR Am J Roentgenol. 2004. 183:1355–1359.21. Wrathall AE, Bailey J, Hebert CN. A radiographic study of development of the appendicular skeleton in the fetal pig. Res Vet Sci. 1974. 17:154–168.22. Connolly SA, Jaramillo D, Hong JK, Shapiro F. Skeletal development in fetal pig specimens: MR imaging of femur with histologic comparison. Radiology. 2004. 233:505–514.23. Kleinman PL, Zurakowski D, Strauss KJ, Cleveland RH, Perez-Rosello JM, Nichols DP, et al. Detection of simulated inflicted metaphyseal fractures in a fetal pig model: image optimization and dose reduction with computed radiography. Radiology. 2008. 247:381–390.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can ultra-low-dose computed tomography reliably diagnose and classify maxillofacial fractures in the clinical routine?
- Ultra-Low-Dose Chest CT in Patients with Neutropenic Fever and Hematologic Malignancy: Image Quality and Its Diagnostic Performance
- Low-dose Hormone Therapy in Postmenopausal Women
- Clinical Comparison of the Predictive Value of the Simple Skull X-Ray and 3 Dimensional Computed Tomography for Skull Fractures of Children
- FLASH Radiotherapy: A FLASHing Idea to Preserve Neurocognitive Function
