Risk Factors for Local Tumor Recurrence after Segmental Transarterial Chemoembolization for Hepatocellular Carcinoma: the Importance of Tumor Located in the Segmental Border Zone
- Affiliations
-
- 1Department of Radiology, Seoul Veterans Hospital, Seoul, Korea.yunkucho2004@yahoo.co.kr
- 2Department of Radiology and Institute of Radiation Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Seoul Veterans Hospital, Seoul, Korea.
- KMID: 1092550
- DOI: http://doi.org/10.3348/kjr.2006.7.4.267
Abstract
OBJECTIVE
We wanted to evaluate whether tumors located in a segmental border zone are predisposed to local recurrence after performing segmental transarterial chemoembolization for hepatocellular carcinoma. MATERIALS AND METHODS: Seventy-three hepatocellular carcinoma nodules were retrospectively analyzed for local tumor recurrence after performing segmental transarterial chemoembolization by using follow-up CT studies (median follow-up period: 20 months, range: 4-77 months). The tumors were divided into two groups according to whether the lesions were located at the segmental border zone (Group I) or not (Group II). Comparison of the tumor characteristics and chemoembolization methods between the two groups was performed using the chi-square test. The local recurrence rates were compared by Kaplan-Meyer method and analyzed with the log rank test. RESULTS: Local tumor recurrence occurred for 25 hepatocellular carcinoma nodules (42.9%). The follow-up periods, tumor characteristics and chemoembolization methods between Groups l and ll were comparable. The local recurrence rate was 64.0% (16/25) in Group I and 18.8% (9/48) in Group II. The difference was statistically significant on the univariate and multivariate analyses (p = 0.000 for both). CONCLUSION: Tumor location in a segmental border zone was a significant risk factor for local tumor recurrence after performing segmental transarterial chemoembolization for hepatocellular carcinoma.
MeSH Terms
-
Risk Factors
Retrospective Studies
Proportional Hazards Models
Neoplasm Recurrence, Local
Middle Aged
Male
Liver Neoplasms/*pathology/*therapy
Iodized Oil/administration & dosage
Humans
Female
Doxorubicin/administration & dosage
Chi-Square Distribution
*Chemoembolization, Therapeutic
Carcinoma, Hepatocellular/*pathology/*therapy
Aged
Adult
Figure
-
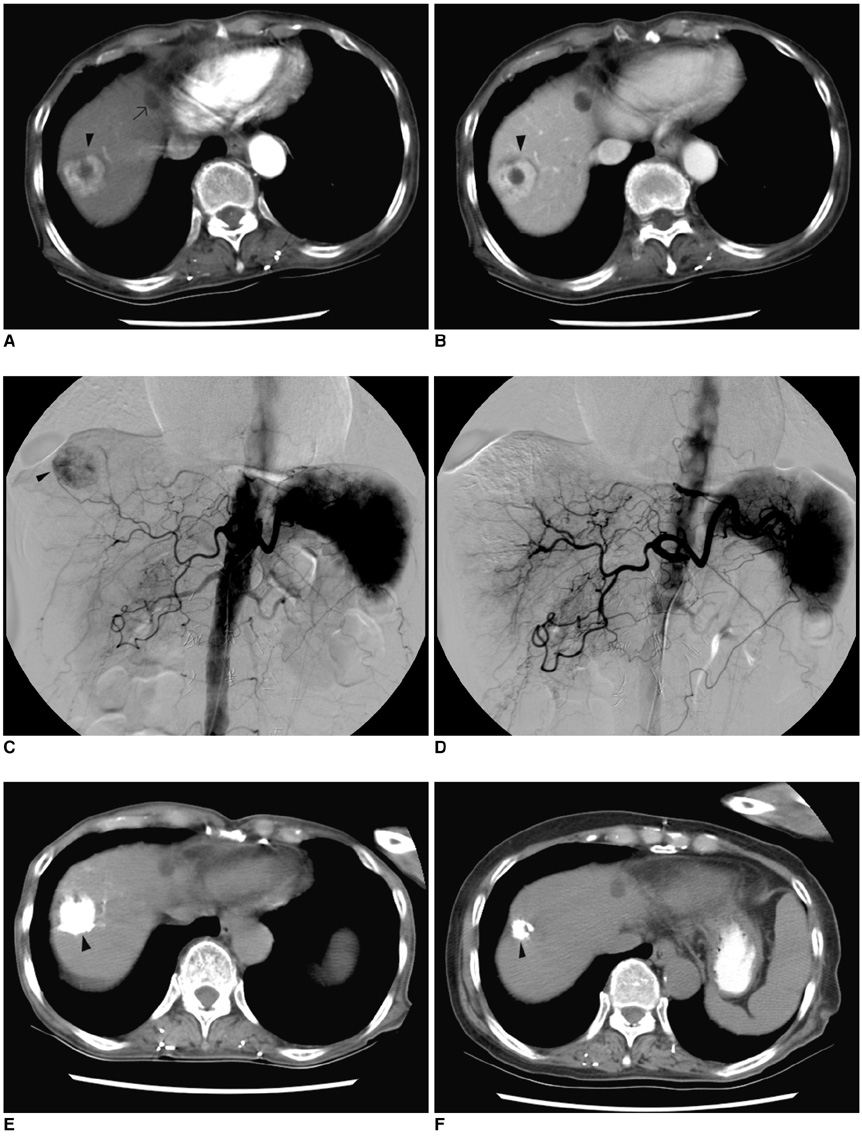
Fig. 1 A 73-year-old woman with hepatocellular carcinoma. A. Pre-embolization CT imaging on the arterial phase reveals a well-defined enhanced mass measuring 2.9 cm in segment 8 of the liver (arrowhead). The low density lesion in the left lobe dome area is a benign cystic lesion without any interval change over a year (arrow). B. Pre-embolization CT imaging on the portal venous phase reveals the same mass with heterogeneous contrast enhancement (arrowhead). C. Pre-embolization hepatic angiogram shows the mass with heterogeneous hypervascularity (arrowhead). D. Post-embolization hepatic angiogram shows the mass without evidence of hypervascular tumor staining. Note that the segmental arterial feeder was also completely occluded. E. One-month follow-up CT imaging shows the mass with inhomogeneous iodized oil accumulation (arrowhead). F. Seven-month follow-up CT imaging reveals the mass with shrinkage (arrowhead). No definite evidence of local tumor recurrence was noted.
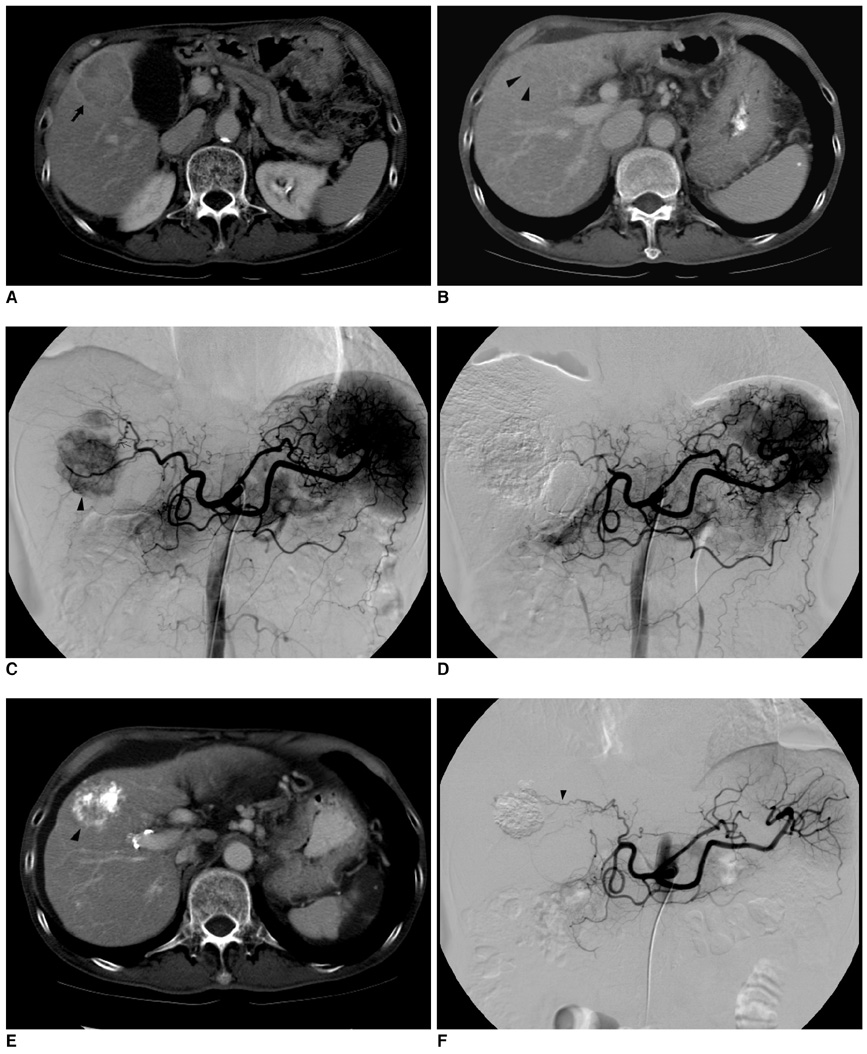
Fig. 2 A 70-year-old man with hepatocellular carcinoma. A. Pre-embolization CT imaging on the portal phase reveals a large well-defined mass measuring 5.1 cm in the S5 segment (arrow). Portal and delayed phase CT imaging (not shown) revealed delayed marginal rim enhancement, which is a typical finding of hepatocellular carcinoma. B. Pre-embolization CT imaging on the portal phase at the level of segmental border zone area between segments 5 and 8. Note that the upper portion of the tumor is also seen at this level (arrowheads). Therefore, this tumor was regarded as located in the segmental border zone between S5 and S8. C. Pre-embolization hepatic angiogram shows the mass with hypervascularity (arrowhead). Note the segmental arterial feeder of the tumor (arrowhead). A minor blood supply to the tumor from the adjacent segmental artery was also confirmed (not shown). D. Post-embolization hepatic angiogram reveals no evidence of residual hypervascular tumor staining. Note that the right hepatic artery is completely occluded. E. One-month follow-up CT imaging shows the mass with inhomogeneous iodized oil accumulation at the segmental border zone of S5 and S8 (arrowhead). The high density area within the tumor was also seen on the precontrast CT imaging (not shown here). F. Seven-month follow-up hepatic angiogram reveals the tumor with local recurrence. Note that the original segmental feeders are completely occluded (arrowheads). Chemoembolization was performed for this mass.
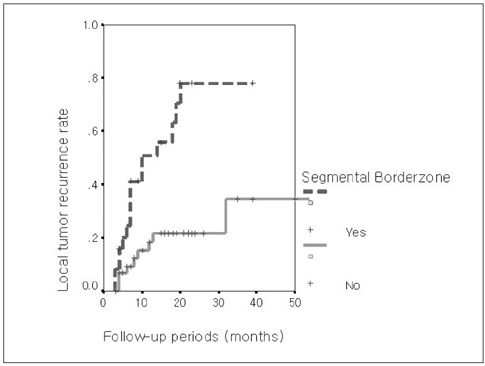
Fig. 3 Comparison of local tumor recurrence rates between tumors located in segmental border zones (n = 25) and those located inside the hepatic segments (n = 48). Tumors located in segmental border zones showed earlier local tumor recurrence compared to those tumors located inside hepatic segments on the univariate and multivariate analyses with using Kaplan-Meyer estimation and the log rank test (p = 0.000 for both).
Reference
-
1. Colella G, Bottelli R, De Carlis L, Sansalone CV, Rondinara GF, Alberti A, et al. Hepatocellular carcinoma: comparison between liver transplantation, resective surgery, ethanol injection, and chemoembolization. Transpl Int. 1998. 11:S193–S196.2. Segawa T, Izawa K, Tsunoda T, Kanematsu T, Shima M, Matsunaga N, et al. Evaluation of hepatectomy in small hepatocellular carcinoma: comparison with transcatheter arterial embolization therapy. Nippon Geka Gakkai Zasshi. 1992. 93:1095–1099.3. Nakamura H, Hashimoto T, Oi H, Sawada S. Transcatheter oil chemoembolization of hepatocellular carcinoma. Radiology. 1989. 170:783–786.4. Bronowicki JP, Vetter D, Dumas F, Boudjema K, Bader R, Weiss AM, et al. Transcatheter oil chemoembolization for hepatocellular carcinoma: A 4-year study of 127 French patients. Cancer. 1994. 74:16–24.5. Uchida H, Ohishi H, Matsuo N, Nishimine K, Ohue S, Nishimura Y, et al. Transcatheter hepatic segmental arterial embolization using lipiodol mixed with anticancer drug and Gelfoam particles for hepatocellular carcinoma. Cardiovasc Intervent Radiol. 1990. 13:140–145.6. Takayasu K, Suzuki M, Uesaka K, Muramatsu Y, Moriyama N, Yoshida T, et al. Hepatic arterial embolization for inoperable hepatocellular carcinoma: prognosis and risk factors. Cancer Chemother Pharmacol. 1989. 23:S123–S125.7. Yamada R, Kishi K, Sonomura T, Tsuda M, Nomura S, Satoh M. Transcatheter arterial embolization in unresectable hepatoellular carcinoma. Cardiovasc Intervent Radiol. 1990. 13:135–139.8. Pelletier G, Rohe A, Ink O, Anciaux ML, Derhy S, Rougier P, et al. A randomized trial of hepatic arterial chemoembolization in patients with unresectable hepatocellular carcinoma. J Hepatol. 1990. 11:181–184.9. Takayasu K, Muramatsu Y, Maeda T, Iwata R, Furukawa H, Muramatsu Y, et al. Targeted transarterial oily chemoembolization for small foci of hepatocellular carcinoma using a unified helical CT and angiography system: analysis of factors affecting local recurrence and survival rates. AJR Am J Roentgenol. 2001. 176:681–688.10. Maeda S, Fujiyama S, Tanaka M, Ashihara H, Hirata R, Tomita K. Survival and local recurrence rates of hepatocellular carcinoma patients treated by transarterial chemolipiodolization with and without embolization. Hepatol Res. 2002. 23:202–210.11. Nguyen M, Garcia R, Simpson P, Wright T, Keeffe E. Racial differences in effectiveness of alpha-fetoprotein for the diagnosis of hepatocellular carcinoma in hepatitis C cirrhosis. Hepatology. 2002. 36:410–417.12. Fischer L, Cardenas C, Thorn M, Benner A, Grenacher L, Lehnert T, et al. Limits of Couinaud's liver segment classification: a quantitative computer-based three-dimensional analysis. J Comput Assist Tomogr. 2002. 26:962–967.13. Choi D, Choo SW, Lim JH, Lee SJ, Do YS, Choo IW. Opacification of the intrahepatic portal veins during CT hepatic arteriography. J Comput Assist Tomogr. 2001. 25:218–224.14. Choi SH, Chung JW, Lee HS. Hepatocellular carcinoma supplied by portal flow after repeated transcatheter arterial chemoembolization. AJR Am J Roentgenol. 2003. 181:889–890.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Local Recurrence of Hepatocellular Carcinoma after Segmental Transarterial Chemoembolization: Risk Estimates Based on Multiple Prognostic Factors
- Hemoperitoneum Secondary to Rupture of Metastatic Hepatocellular Carcinoma : A Case Report
- Complete Remission with Transarterial Chemoembolization in a Patient with Hepatocellular Carcinoma Who Showed Early Recurrence following Surgical Resection
- Aggressive tumor recurrence after radiofrequency ablation for hepatocellular carcinoma
- Rupture of hepatocellular carcinoma after transcatheter arterial chemoembolization: A case report
