Korean J Ophthalmol.
2011 Dec;25(6):417-420. 10.3341/kjo.2011.25.6.417.
Attempts to Reduce the Progression of Myopia and Spectacle Prescriptions during Childhood: A Survey of Eye Specialists
- Affiliations
-
- 1Department of Ophthalmology, Kim's Eye Hospital, Konyang University College of Medicine, Seoul, Korea. ungsookim@kimeye.com
- KMID: 1031189
- DOI: http://doi.org/10.3341/kjo.2011.25.6.417
Abstract
- PURPOSE
To determine methods tried in clinical trials to reduce the progression of myopia in children, and spectacle prescribing patterns of hospital ophthalmologists.
METHODS
A multi-sectioned survey composed of Likert items relating to the methods of reducing myopia progression (orthokeratology lenses [O-K lenses], undercorrected glasses, and topical atropine) and the patterns of prescribing spectacles for children (including two cases involving a 5-year-old girl and an 8-year-old boy) were distributed to members of the Korean Ophthalmological Society, and the collected data was statistically analyzed.
RESULTS
A total of 78 out of 130 ophthalmologists returned the survey. On a scale of 1 to 5, the mean rates of whether the ophthalmologists think O-K lenses arrest myopia progression, and whether they recommend their patients to wear O-K lenses if indicative, were 3.06 and 2.75, respectively. Moreover, the mean rates of whether they consider that wearing glasses which are undercorrected would slow down the progression of the myopia, or if they think topical atropine helps in arresting myopia progression in children, were 2.34 and 1.27, respectively. In response to the case studies, the majority of practitioners preferred to prescribe the full amount found in cycloplegic refraction to pediatric patients with myopia.
CONCLUSIONS
Ophthalmologists in clinical practice encouraged children to wear O-K lenses more than undercorrected glasses as a way to retard myopia progression. However, the application of atropine is rarely tried in clinical trials. In managing pediatric patients with myopia (case specific), the majority of the practitioners chose to prescribe glasses with full cycloplegic correction.
Keyword
MeSH Terms
-
Atropine/administration & dosage
Child
Child, Preschool
Data Collection
Disease Progression
Eyeglasses/classification/*utilization
Female
Health Knowledge, Attitudes, Practice
Humans
Male
Myopia/physiopathology/*prevention & control
Physician's Practice Patterns
Prescriptions/*statistics & numerical data
Republic of Korea
Figure
-
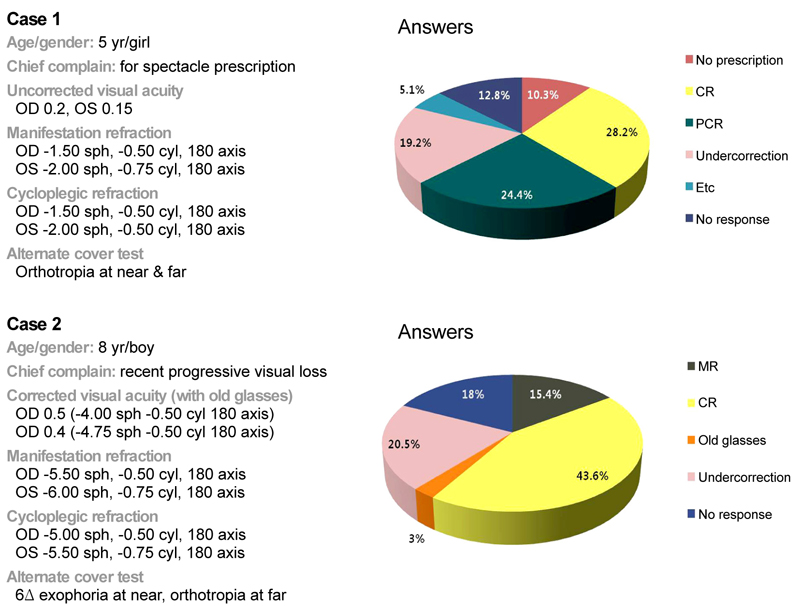
Fig. 1 Detailed description of case 1 and 2 and the answers for preferred spectacle prescription of case 1 and 2. OD = right eye; OS = left eye; CR = cycloplegic refraction; PCR = post-cycloplegic refraction; MR = manifestation refraction.
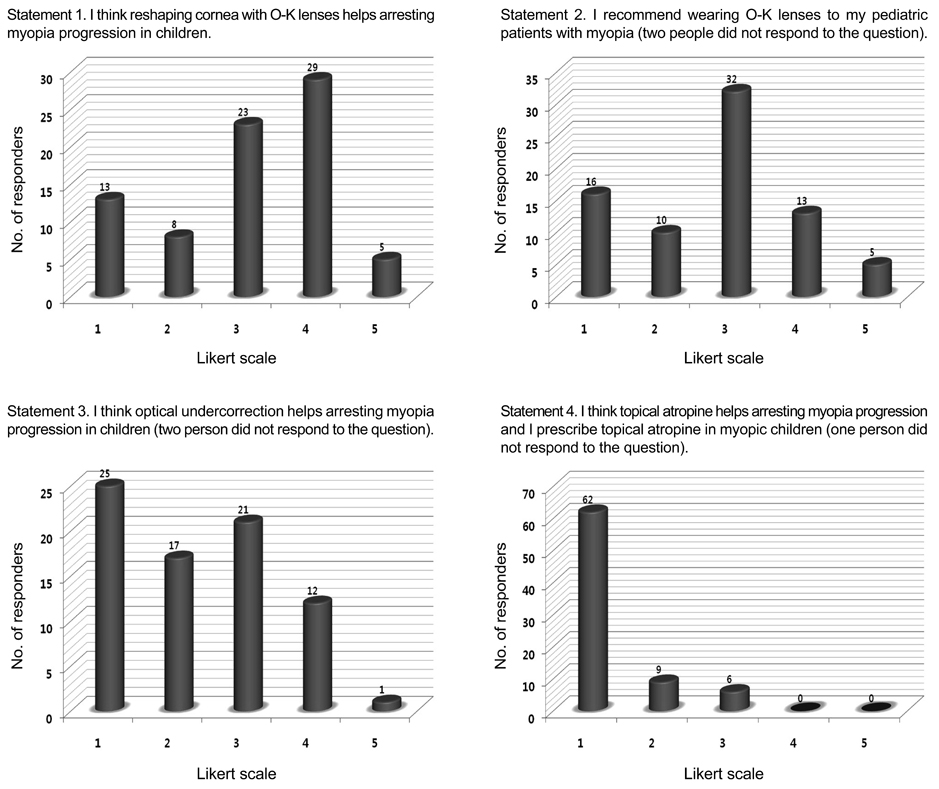
Fig. 2 Analysis of the survey results about the prevention of myopic progression. Likert scale - 1, strongly disagree; 2, disagree; 3, unsure; 4, agree; 5, strongly agree. O-K lenses = orthokeratology lenses.
Reference
-
1. Saw SM, Tong L, Chua WH, et al. Incidence and progression of myopia in Singaporean school children. Invest Ophthalmol Vis Sci. 2005. 46:51–57.2. Goldschmidt E. The mystery of myopia. Acta Ophthalmol Scand. 2003. 81:431–436.3. Lin LL, Shih YF, Tsai CB, et al. Epidemiologic study of ocular refraction among schoolchildren in Taiwan in 1995. Optom Vis Sci. 1999. 76:275–281.4. Saw SM, Katz J, Schein OD, et al. Epidemiology of myopia. Epidemiol Rev. 1996. 18:175–187.5. Saw SM, Hong RZ, Zhang MZ, et al. Near-work activity and myopia in rural and urban schoolchildren in China. J Pediatr Ophthalmol Strabismus. 2001. 38:149–155.6. Chan B, Cho P, Cheung SW. Orthokeratology practice in children in a university clinic in Hong Kong. Clin Exp Optom. 2008. 91:453–460.7. Heng LS, Khoo CY. Can contact lenses control the progression of myopia? Singapore Med J. 1994. 35:367–370.8. Rubin ML, Milder B. Myopia--a treatable "disease"? Surv Ophthalmol. 1976. 21:65–69.9. Bedrossian RH. The effect of atropine on myopia. Ann Ophthalmol. 1971. 3:891–897.10. Choi TH, Jeong JW, Choi YY. The effect of atropine on myopic progression in children. J Korean Ophthalmol Soc. 2005. 46:1189–1195.11. Adler D, Millodot M. The possible effect of undercorrection on myopic progression in children. Clin Exp Optom. 2006. 89:315–321.12. Gwiazda J. Treatment options for myopia. Optom Vis Sci. 2009. 86:624–628.13. Saw SM, Gazzard G, Au Eong KG, Tan DT. Myopia: attempts to arrest progression. Br J Ophthalmol. 2002. 86:1306–1311.14. Syniuta LA, Isenberg SJ. Atropine and bifocals can slow the progression of myopia in children. Binocul Vis Strabismus Q. 2001. 16:203–208.15. Van Meter WS, Musch DC, Jacobs DS, et al. Safety of overnight orthokeratology for myopia: a report by the American Academy of Ophthalmology. Ophthalmology. 2008. 115:2301–2313.e1.16. McLeod SD. Overnight orthokeratology and corneal infection risk in children. Arch Ophthalmol. 2007. 125:688–689.17. Chung K, Mohidin N, O'Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res. 2002. 42:2555–2559.18. Tong L, Huang XL, Koh AL, et al. Atropine for the treatment of childhood myopia: effect on myopia progression after cessation of atropine. Ophthalmology. 2009. 116:572–579.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention of myopia progression using orthokeratology
- The Progression of Myopia with Age
- Progression of Myopia in the Patients with Astigmatism over 3.0 Diopters
- Impact of Myopia Progression and Its Intervention Methods on Choroidal Thickness
- Excimer laser Radial Keratotomy for Correction of Myopia and Astigmatism: Preliminary Report
