Imaging Findings in a Case of Mixed Acinar-Endocrine Carcinoma of the Pancreas
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 138-736, Korea. jhbyun@amc.seoul.kr
- KMID: 946281
- DOI: http://doi.org/10.3348/kjr.2010.11.3.378
Abstract
- Mixed acinar-endocrine carcinoma (MAEC) of the pancreas is extremely uncommon. We report here a rare case of MAEC of the pancreas presenting as watery diarrhea. This is the first report in the English-language literature that describes the imaging findings of MAEC of the pancreas, including computed tomography (CT), magnetic resonance (MR) imaging, and MR cholangiopancreatography features.
MeSH Terms
-
Carcinoma, Acinar Cell/*pathology/*radiography/surgery
Cholangiopancreatography, Magnetic Resonance/methods
Diagnosis, Differential
Diarrhea
Endocrine Gland Neoplasms/*pathology/*radiography/surgery
Female
Humans
Magnetic Resonance Imaging/methods
Middle Aged
Pancreas/pathology/radiography/surgery
Pancreatectomy
Pancreatic Neoplasms/*pathology/*radiography/surgery
Splenectomy
Tomography, X-Ray Computed/methods
Figure
-
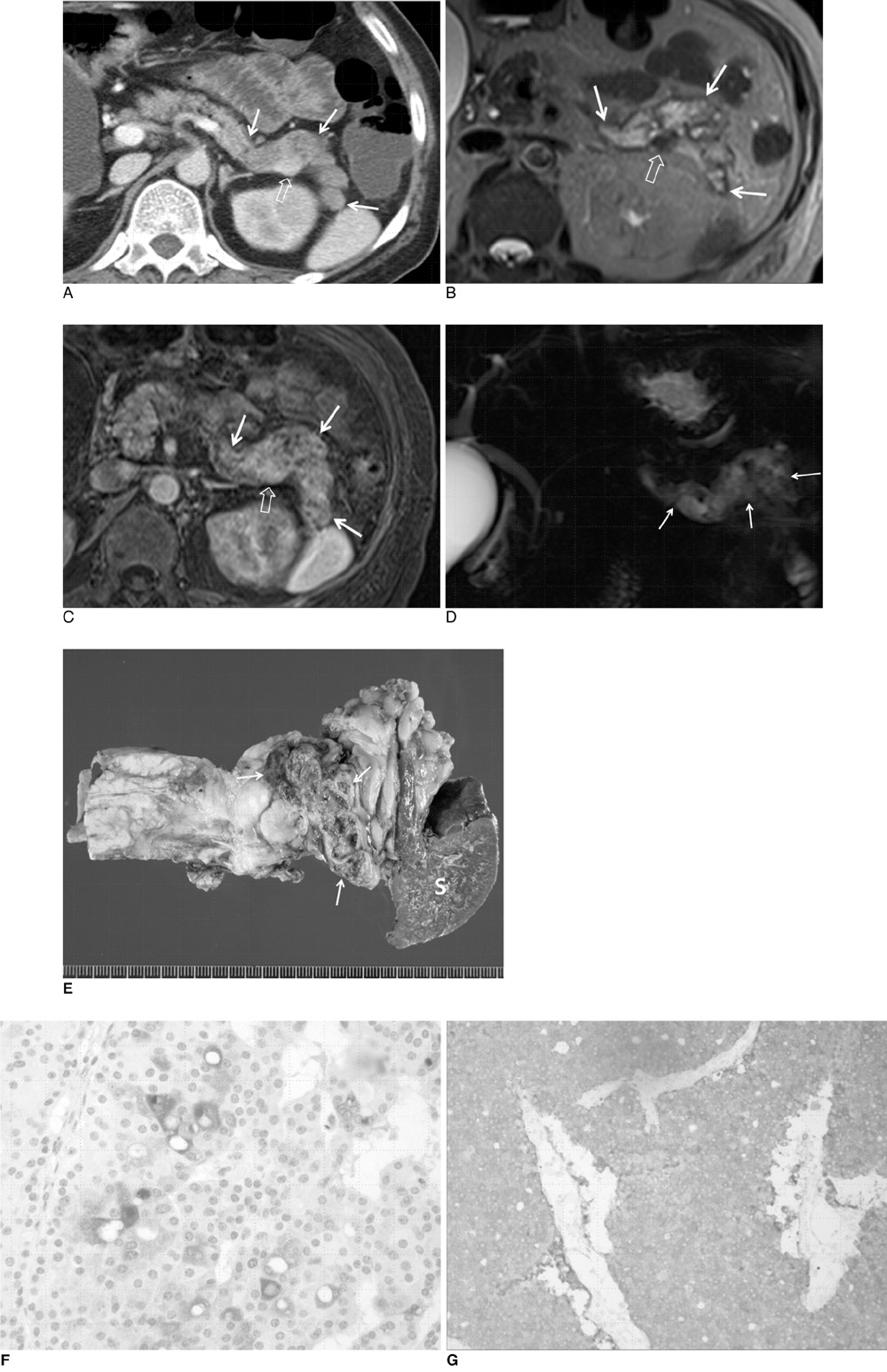
Fig. 1 59-year-old woman presented with watery diarrhea that had persisted for two years. A. On contrast-enhanced axial CT scan during hepatic arterial phase, tail of pancreas, which is approximately half length of longest pancreatic axis, was diffusely replaced by heterogeneously hypo-attenuating mass-like lesion (arrows). Approximately 1.5-cm hypervascular nodule (open arrow) was also visible in mass. B. T2-weighted axial MR image indicates that mass (arrows) was heterogeneously hyperintense compared to normal pancreas, except for heterogeneously hypointense nodule (open arrow) in mass. C. Contrast-enhanced T1-weighted axial MR image during hepatic arterial phase showed that tumor (arrows) enhances heterogeneously with multiple well or poorly enhancing areas relative to normal pancreas. Nodule (open arrow) in mass was also found to be well enhanced. D. MR cholangiopancreatography showed that tumor (arrows) was hyperintense with multiple hypointense nodular lesions. E. Photograph of surgical specimen reveals well-demarcated, lobulate, soft-tissue mass (arrows) located at tail of pancreas. Areas of hemorrhage and focal necrosis with cystic change in mass are evident. S = spleen F. Immunohistochemistry results suggest that tumor cells are immunoactive for anti-trypsin (×200). G. Photomicrograph of mass with immunohistochemical staining showed that tumor cells are immunoactive for synaptophysin (×100).
Reference
-
1. Kamisawa T, Tu Y, Egawa N, Ishiwata J, Tsuruta K, Okamoto A, et al. Ductal and acinar differentiation in pancreatic endocrine tumors. Dig Dis Sci. 2002. 47:2254–2261.2. Klöppel G. Mixed exocrine-endocrine tumors of the pancreas. Semin Diagn Pathol. 2000. 17:104–108.3. Schron DS, Mendelsohn G. Pancreatic carcinoma with duct, endocrine, and acinar differentiation. A histologic, immunocytochemical, and ultrastructural study. Cancer. 1984. 54:1766–1770.4. Ohike N, Kosmahl M, Klöppel G. Mixed acinar-endocrine carcinoma of the pancreas. A clinicopathological study and comparison with acinar-cell carcinoma. Virchows Arch. 2004. 445:231–235.5. Cubilla AL, Fitzgerald PJ. Cancer of the exocrine pancreas: the pathologic aspects. CA Cancer J Clin. 1985. 35:2–18.6. Yantiss RK, Chang HK, Farraye FA, Compton CC, Odze RD. Prevalence and prognostic significance of acinar cell differentiation in pancreatic endocrine tumors. Am J Surg Pathol. 2002. 26:893–901.7. Ballas KD, Rafailidis SF, Demertzidis C, Alatsakis MB, Pantzaki A, Sakadamis AK. Mixed exocrine-endocrine tumor of the pancreas. JOP. 2005. 6:449–454.8. Klimstra DS, Rosai J, Heffess CS. Mixed acinar-endocrine carcinomas of the pancreas. Am J Surg Pathol. 1994. 18:765–778.9. Cubilla A, Fitzgerald PJ. Pancreas cancer. I. Duct adenocarcinoma. A clinical-pathologic study of 380 patients. Pathol Annu. 1978. 13:241–389.10. Clark LR, Jaffe MH, Choyke PL, Grant EG, Zeman RK. Pancreatic imaging. Radiol Clin North Am. 1985. 23:489–501.11. Choi YJ, Byun JH, Kim JY, Kim MH, Jang SJ, Ha HK, et al. Diffuse pancreatic ductal adenocarcinoma: characteristic imaging features. Eur J Radiol. 2008. 67:321–328.12. Pamuklar E, Semelka RC. MR imaging of the pancreas. Magn Reson Imaging Clin N Am. 2005. 13:313–330.13. Choi EK, Park SH, Kim DY, Kim KW, Byun JH, Lee MG, et al. Unusual manifestations of primary pancreatic neoplasia: radiologic-pathologic correlation. J Comput Assist Tomogr. 2006. 30:610–617.14. Tatli S, Mortele KJ, Levy AD, Glickman JN, Ros PR, Banks PA, et al. CT and MRI features of pure acinar cell carcinoma of the pancreas in adults. AJR Am J Roentgenol. 2005. 184:511–519.15. Merkle EM, Bender GN, Brambs HJ. Imaging findings in pancreatic lymphoma: differential aspects. AJR Am J Roentgenol. 2000. 174:671–675.16. Klein KA, Stephens DH, Welch TJ. CT characteristics of metastatic disease of the pancreas. Radiographics. 1998. 18:369–378.
