A Case of Caroli Disease with Biliary Stones
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. gidoctor@snubh.org
- 2Department of Radiology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Pathology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 783224
- DOI: http://doi.org/10.4166/kjg.2009.54.4.201
Abstract
- No abstract available.
MeSH Terms
Figure
-
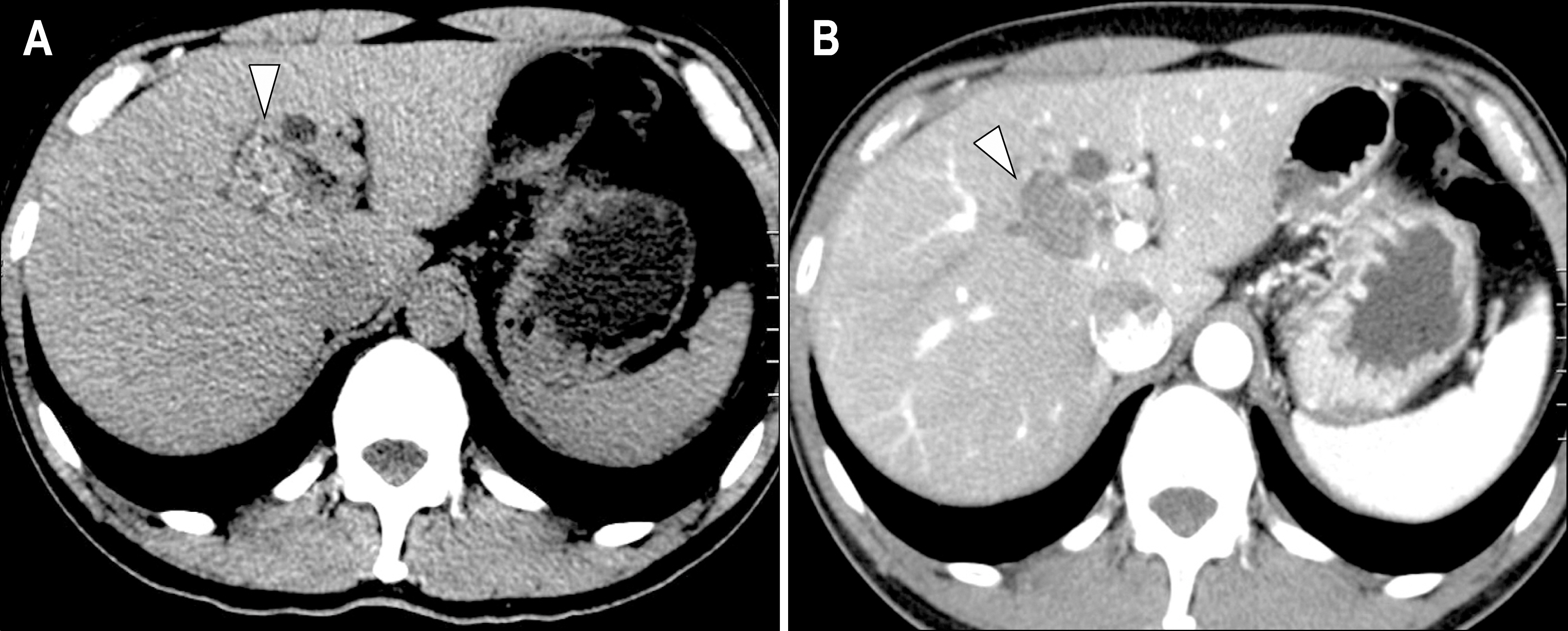
Fig. 1. Pancreatico-bliliary CT and MRCP findings. (A) Non-contrast image. In segment IV/VIII of left lobe of liver, multiple high attenuated stones were found (arrowhead). (B) Contrast-enhanced image. This image showed focal low attenuated cystic dilatation of right intrahepatic duct (arrowhead). It also showed no definite dilatation of intrahepatic duct in other segments of the liver.
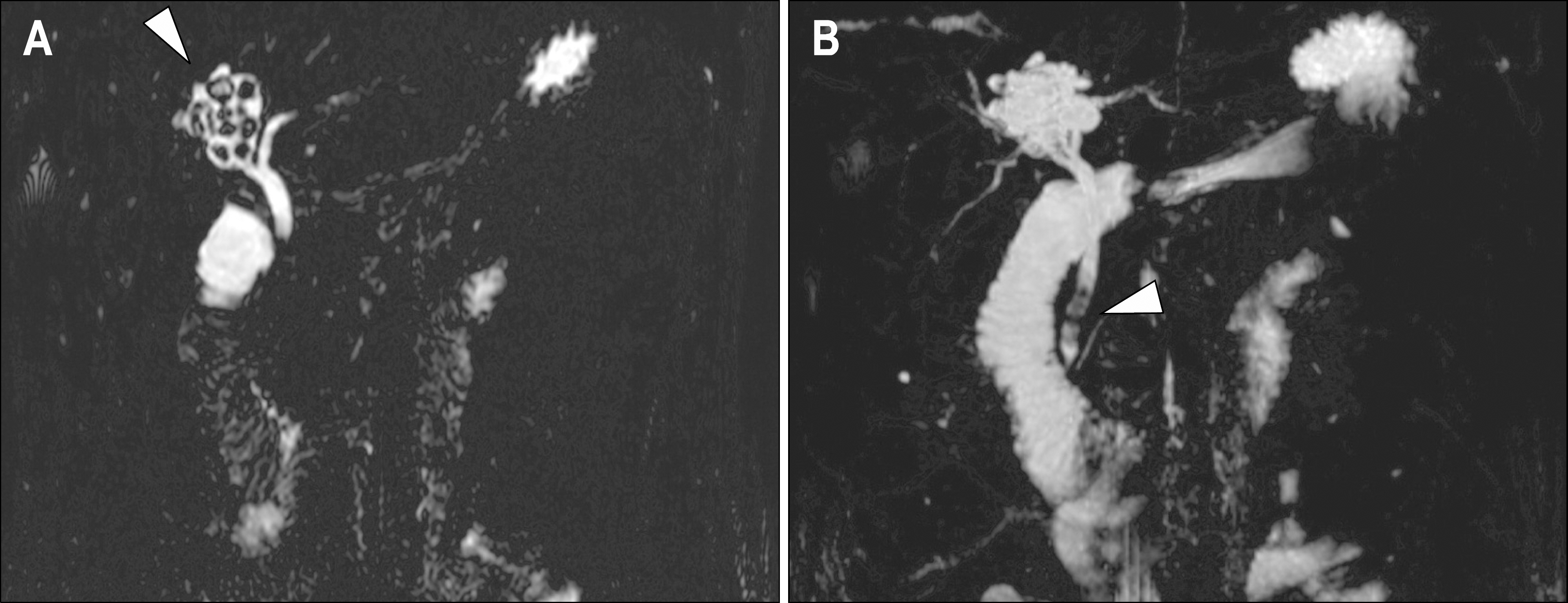
Fig. 2. MRCP findings. (A) T2-weighted image. MRCP image showed a cystic dilatation of IHD containing multiple stones, adjacent to the right hepatic duct (arrowhead). (B) T2-weighted image. There were multiple filling defects which reflected stones in distal common bile duct (arrowhead).
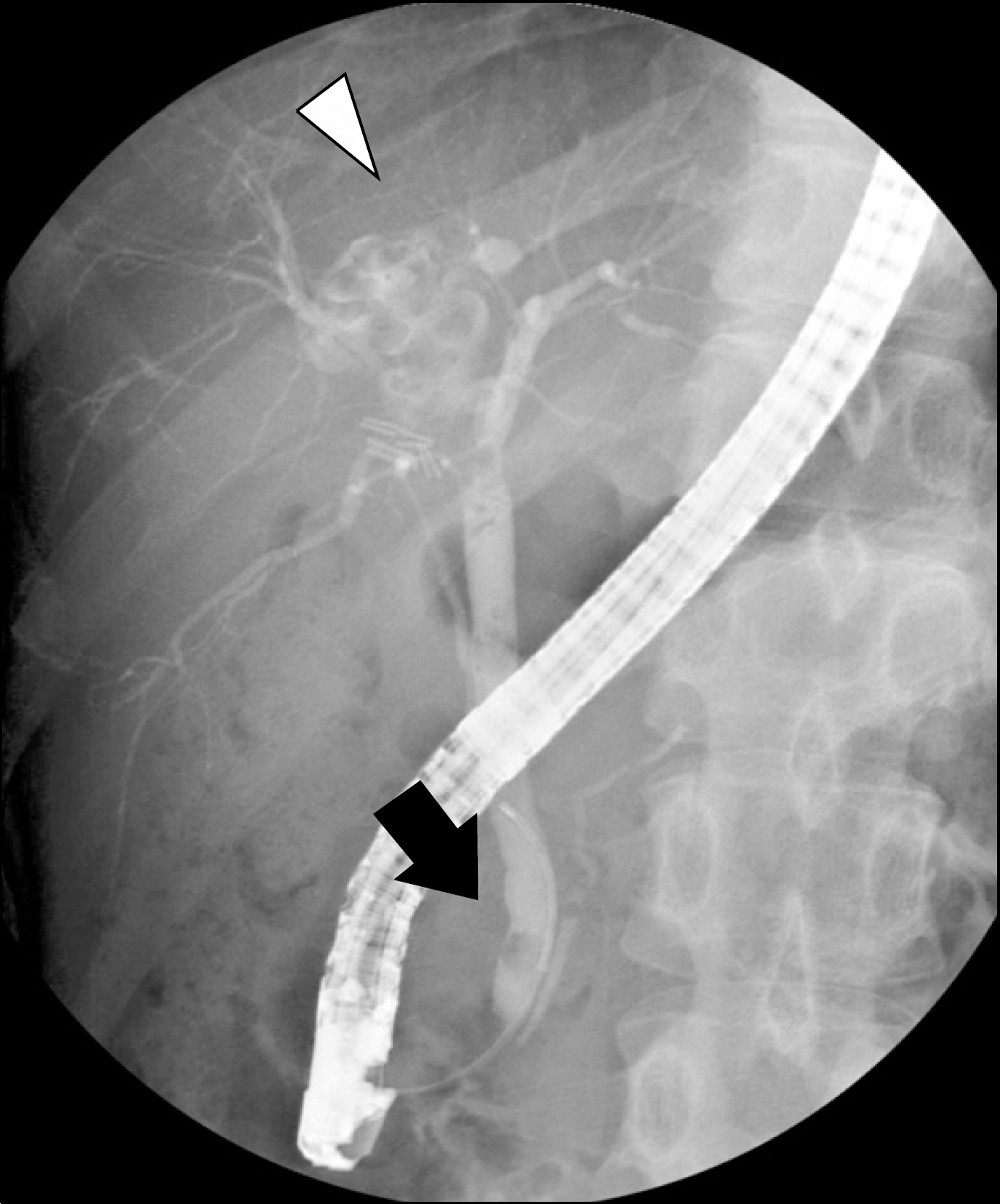
Fig. 3. ERCP finding showed cystic dilatation of IHD in right hepatic duct with multiple filling defects due to stones (arrowhead). This cystic lesion had communication with common hepatic duct, significant features to diagnose as Caroli's diseas. It also had some defects suggesting distal common bile duct stones (arrow). In this procedure, brown pigmented stone was removed with retrieval basket successfully.

Fig. 4. Pathological findings. (A) Gross examination of the specimen demonstrated cystic dilatation of the bile duct. (B-D) The bile duct wall showed fibrous thickening, chronic inflammation, and denudation of the surface epithelial lining. A small focus of remaining epithelium was noted (D, arrowheads) (B-D: Hematoxylin-Eosin; original magnification ×10 (B), ×40 (C) and ×100 (D)).
Reference
-
1. Caroli J, Couinaud C, Soupault R, Porcher P, Eteve J. A new disease, undoubtedly congenital, of the bile ducts: unilobar cystic dilation of the hepatic ducts. Sem Hop. 1958; 34:496–502. /SP.2. Giovanardi RO. Monolobar Caroli's disease in an adult. Case report. Hepatogastroenterology. 2003; 50:2185–2187.3. Parada LA, Hallen M, Hagerstrand I, Tranberg KG, Johansson B. Clonal chromosomal abnormalities in congenital bile duct dilatation (Caroli's disease). Gut. 1999; 45:780–782.
Article4. Levy AD, Rohrmann CA Jr, Murakata LA, Lonergan GJ. Caroli's disease: radiologic spectrum with pathologic correlation. AJR Am J Roentgenol. 2002; 179:1053–1057.
Article5. Asselah T, Ernst O, Sergent G, L'Hermine C, Paris JC. Caroli's disease: a magnetic resonance cholangiopancreatography diagnosis. Am J Gastroenterol. 1998; 93:109–110.
Article6. Yilmaz S, Kirimlioglu H, Kirimlioglu V, et al. Partial hepatectomy is curative for the localized type of Caroli's disease: a case report and review of the literature. Surgeon. 2006; 4:101–105.
Article7. Bockhorn M, Malago M, Lang H, et al. The role of surgery in Caroli's disease. J Am Coll Surg. 2006; 202:928–932.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diffuse-Type Caroli Disease with Characteristic Central Dot Sign Complicated by Multiple Intrahepatic and Common Bile Duct Stones
- Unexpectedly Diagnosed Caroli's Disease on HIDA Scintigraphy in a Patient with Calculous Cholecystitis
- Monolobar Caroli's Disease in Left Lobe of the Liver: A Case Report
- A case of Caroli's disease
- A Case Report of Caroli's Disease
