Diffuse-Type Caroli Disease with Characteristic Central Dot Sign Complicated by Multiple Intrahepatic and Common Bile Duct Stones
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea. tnkim@yu.ac.kr
- KMID: 2389247
- DOI: http://doi.org/10.5946/ce.2016.150
Abstract
- Caroli disease (CD) is a rare congenital malformation of the liver characterized by non-obstructive, segmental, cystic dilatation of the intrahepatic bile ducts (IHDs). The clinical course is usually asymptomatic for the first 5-20 years, and symptoms may seldom occur throughout the patient's life. Bile stagnation leads to recurrent episodes of cholangitis, stone formation, or liver abscesses, and biliary cirrhosis usually occurs years later. Here we report on a 42-year-old man diagnosed with diffuse-type CD with a characteristic central dot sign, who had multiple intrahepatic and common bile duct (CBD) stones. CBD stones were treated successfully with endoscopic retrograde cholangiopancreatography (ERCP).
Keyword
MeSH Terms
Figure
-
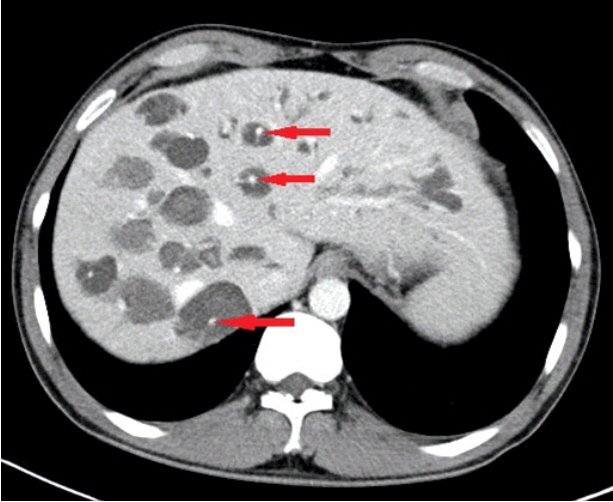
Fig. 1. Abdominal computed tomography. Multiple dilated intrahepatic ducts with tiny dots of strong contrast are seen in the liver (arrows). These represent portal radicles and constitute the characteristic central dot sign for Caroli disease.
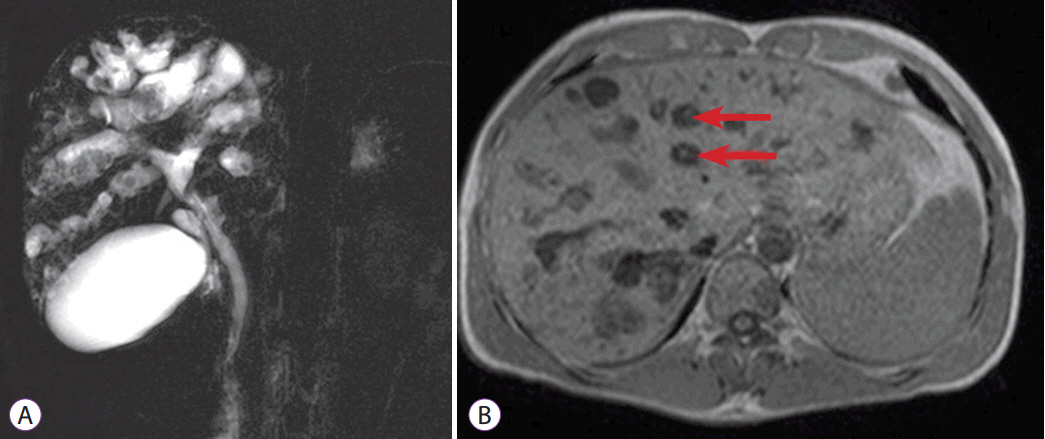
Fig. 2. Magnetic resonance cholangiography. (A) Bile duct ectasia and irregular cystic dilation of the large proximal intrahepatic bile duct (IHD) with a normal common bile duct are noted. Multiple intrahepatic calculi were also demonstrated. (B) T1-weighted image again reveals central dot signs (arrows), which are enhancing dots within the dilated IHD, representing portal radicles (B).

Fig. 3. Endoscopic retrograde cholangiopancreatography. (A) Multiple small cystic formations, in intimate anatomical association with biliary branches were demonstrated. Minimum amount of contrast dye was injected to prevent cholangitis. (B) Black pigment stone was removed by basket method.
Reference
-
1. Caroli J, Couinaud C, Soupault R, Porcher P, Eteve J. [A new disease, undoubtedly congenital, of the bile ducts: unilobar cystic dilation of the hepatic ducts]. Sem Hop. 1958; 34:496–502/SP.2. Giovanardi RO. Monolobar Caroli’s disease in an adult. Case report. Hepatogastroenterology. 2003; 50:2185–2187.3. Pezzilli R, Carini G, Cennamo V. Education and imaging. Hepatobiliary and pancreatic: Caroli’s disease. J Gastroenterol Hepatol. 2008; 23:1621.4. Gupta AK, Gupta A, Bhardwaj VK, Chansoria M. Caroli’s disease. Indian J Pediatr. 2006; 73:233–235.
Article5. Levy AD, Rohrmann CA Jr, Murakata LA, Lonergan GJ. Caroli’s disease: radiologic spectrum with pathologic correlation. AJR Am J Roentgenol. 2002; 179:1053–1057.
Article6. Desmet VJ. Ludwig symposium on biliary disorders--part I. Pathogenesis of ductal plate abnormalities. Mayo Clin Proc. 1998; 73:80–89.
Article7. Yonem O, Bayraktar Y. Clinical characteristics of Caroli’s disease. World J Gastroenterol. 2007; 13:1930–1933.
Article8. Chae YJ, Choi CY, Kim JY, et al. Caroli’s disease combined with colon cancer and polycystic kidney disease. Korean J Gastrointest Endosc. 2006; 32:71–74.9. Wang ZX, Li YG, Wang RL, et al. Clinical classification of Caroli’s disease: an analysis of 30 patients. HPB (Oxford). 2015; 17:278–283.
Article10. Bockhorn M, Malagó M, Lang H, et al. The role of surgery in Caroli’s disease. J Am Coll Surg. 2006; 202:928–932.
Article11. Chapman RW. Risk factors for biliary tract carcinogenesis. Ann Oncol. 1999; 10 Suppl 4:308–311.
Article12. Dayton MT, Longmire WP Jr, Tompkins RK. Caroli’s disease: a premalignant condition? Am J Surg. 1983; 145:41–48.
Article13. Totkas S, Hohenberger P. Cholangiocellular carcinoma associated with segmental Caroli’s disease. Eur J Surg Oncol. 2000; 26:520–521.
Article14. Shimonishi T, Sasaki M, Nakanuma Y. Precancerous lesions of intrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Surg. 2000; 7:542–550.
Article15. Lall NU, Hogan MJ. Caroli disease and the central dot sign. Pediatr Radiol. 2009; 39:754.
Article16. Chung EM, Conran RM, Schroeder JW, Rohena-Quinquilla IR, Rooks VJ. From the radiologic pathology archives: pediatric polycystic kidney disease and other ciliopathies: radiologic-pathologic correlation. Radiographics. 2014; 34:155–178.
Article17. Sinakos E, Papalavrentios L, Chourmouzi D, Dimopoulou D, Drevelegas A, Akriviadis E. The clinical presentation of von Meyenburg complexes. Hippokratia. 2011; 15:170–173.18. Ros E, Navarro S, Bru C, Gilabert R, Bianchi L, Bruguera M. Ursodeoxycholic acid treatment of primary hepatolithiasis in Caroli’s syndrome. Lancet. 1993; 342:404–406.
Article19. Gu DH, Park MS, Jung CH, et al. Caroli’s disease misdiagnosed as intraductal papillary neoplasm of the bile duct. Clin Mol Hepatol. 2015; 21:175–179.
Article20. Ulrich F, Steinmüller T, Settmacher U, et al. Therapy of Caroli’s disease by orthotopic liver transplantation. Transplant Proc. 2002; 34:2279–2280.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Monolobar Caroli's Disease in Left Lobe of the Liver: A Case Report
- Solitary intrahepatic bile-duct cyst presenting with jaundice
- Actinomycosis of the intrahepatic bile duct concomitant with intrahepatic duct stones
- Ultrasonographic findings of intrahepatic bile duct stone
- Application of Electrohydraulic Lithotripsy for Bile Duct Stones Difficult to Remove
