The Efficacy of Metallic Stent Placement in the Treatment of Colorectal Obstruction
- Affiliations
-
- 1Department of Diagnostic Radiology, Chosun University Medical College, Korea. gangsg@mail.chosun.ac.kr
- 2Department of Diagnostic Radiology, Goshin University Medical College, Korea.
- 3Department of Diagnostic Radiology, Inha University Medical College, Korea.
- 4Department of Diagnostic Radiology, Chonnam University Medical College, Korea.
- 5Department of Diagnostic Radiology, Gyonghee University Medical College, Korea.
- 6Department of Diagnostic Radiology, Ulsan University Medical College, Korea.
- 7S & G Biotech, Inc.
- KMID: 754066
- DOI: http://doi.org/10.3348/kjr.2002.3.2.79
Abstract
- DBJECTIVE: To evaluate the efficacy of newly designed covered and non-covered coated colorectal stents for colonic decompression.
MATERIALS AND METHODS
Twenty-six patients, (15 palliative cases and 11 preoperative) underwent treatment for the relief of colorectal obstruction using metallic stents positioned under fluoroscopic guidance. In 24 of the 26, primary colorectal carcinoma was diagnosed, and in the remaining two, recurrent colorectal carcinoma. Twenty-one patients were randomly selected to receive either a type A or type B stent; for the remaining five, type C was used. Type A, an uncovered nitinol wire stent, was lightly coated to ensure structural integrity. Type B (flare type) and C (shoulder type) stents were polyurethane covered and their diameter was 24 and 26mm, respectively. The rates of technical success, clinical success, and complications were analyzed using the chi-square test, and to analyse the mean period of patency, the Kaplan-Meier method was used.
RESULTS
Thirty of 31 attempted placements in 26 patients were successful, with a technical success rate of 96.8% (30/31) and a clinical success rate of 80.0% (24/30). After clinically successful stent placement, bowel decompression occurred within 1-4 (mean, 1.58+/-0.9) days. Five of six clinical failures involved stent migration and one stent did not expand after successful placement. In the preoperative group, 11 stents, one of which migrated, were placed in ten patients, in all of whom bowel preparation was successful. In the palliative group, 19 stents were placed in 15 patients. The mean period of patency was 96.25+/-105.12 days: 146.25+/-112.93 for type-A, 78.82+/-112.26 for type-B, and 94.25+/-84.21 for type-C. Complications associated with this procedure were migration (n=6, 20%), pain (n=4, 13.3%), minor bleeding (n=5, 16.7%), incomplete expansion (n=1, 3.3%), and tumor ingrowth (n=1, 3.3%). The migration rate was significantly higher in the type-B group than in other groups (p=0.038).
CONCLUSION
Newly designed covered and non-covered metallic stents of a larger diameter are effective for the treatment of colorectal obstruction. The migration rate of covered stents with flaring is higher than that of other types. For evaluation of the ideal stent configuration for the relief of colorectal obstruction, a clinical study involving a larger patient group is warranted.
Keyword
MeSH Terms
Figure
-
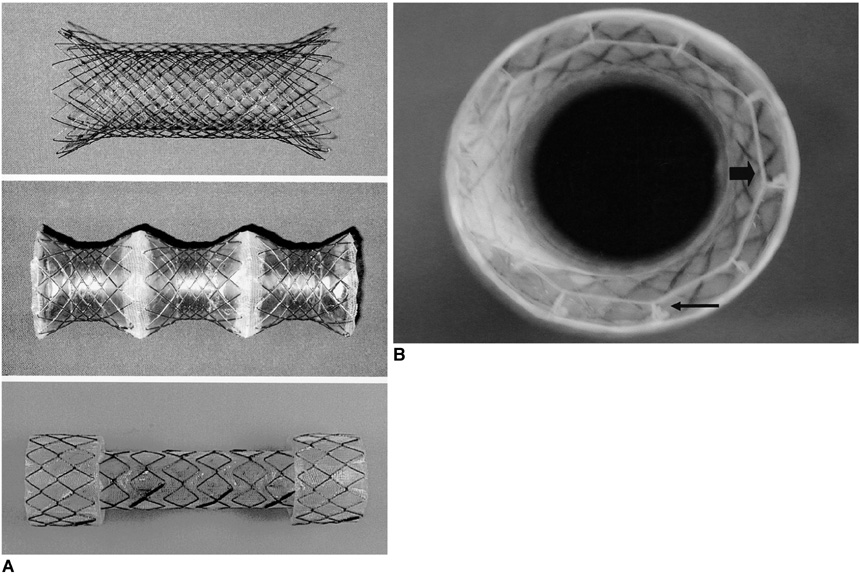
Fig. 1 A. Three types of colorectal stent: type A (upper), type B (middle), and type C (lower). B. The drawstring. Each bend of each segment contains a 2-mm-diameter nylon monofilament loop secured with sutures (thin arrow). These loops form the anchor for another nylon thread which is passed through each of them to form a large loop or drawstring (thick arrow) that fills the inner circumference of the inside of the proximal stent. The resultant loop is then tied at the stent's upper inner margin.
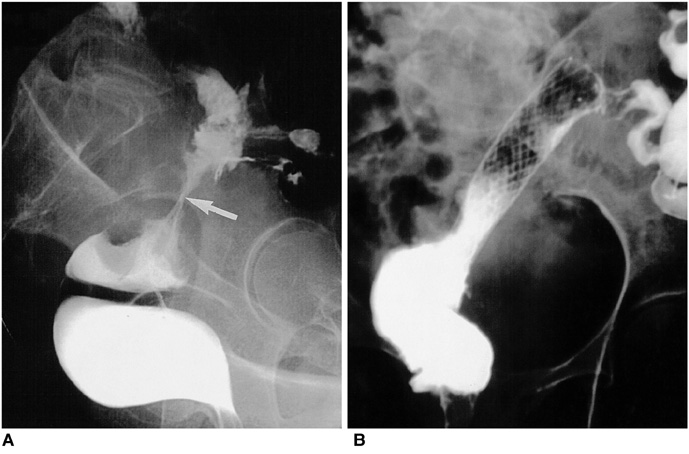
Fig. 2 Type-A stent placement for presurgical bowel preparation (patient #10). A. Irregular narrowing of the proximal rectum (arrow) is apparent. B. Although focal narrowing remains, good passage of contrast medium is observed after type-A stent placement. Four days after placement, this patient underwent anastomosis and tumor resection.

Fig. 3 Type-B stent placement for palliation (patient #8). A. Irregular narrowing of the rectosigmoid colon (arrow) can be seen. B. After type-B stent placement, good patency is observed (arrow). In this patient, symptoms of obstruction recurred 180 days after placement, and a palliative ileostomy was performed.
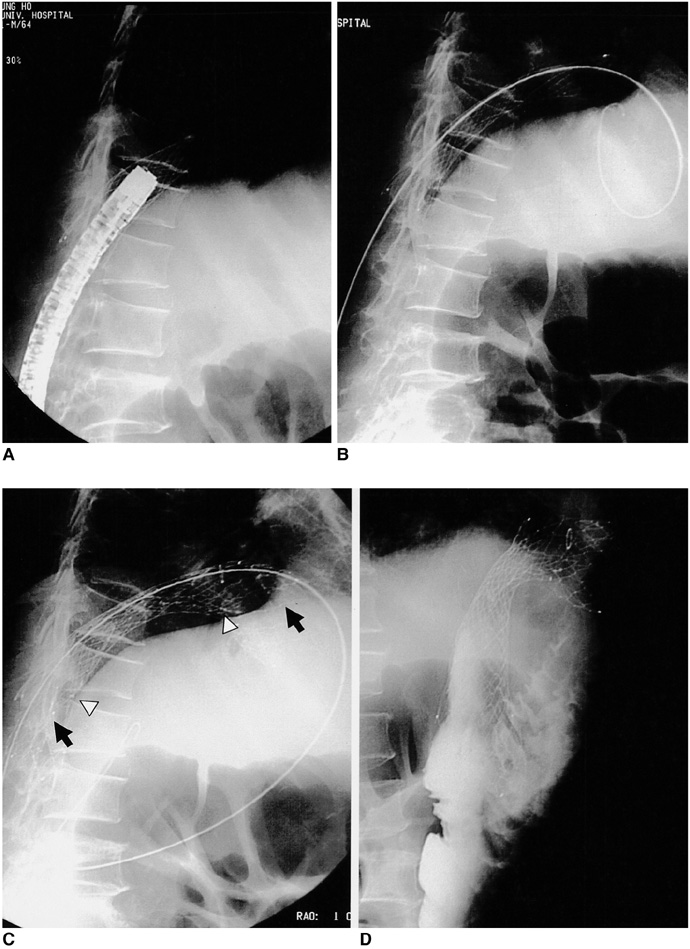
Fig. 4 Type-C stent placement inside a type-A stent (patient #21). A. Tumor ingrowth, which developed four months after stent placement, was confirmed by endoscopy. B. Guidewire advanced through previously placed type-A stent. C. Deployment of type-C stent (arrow), which is longer than type A (arrowheads). D. The type-C stent showed good patency and was patent for three months, until the patient's death.
Reference
-
1. Camunez F, Echenagusia A, Simo G, Turegano F, Vazquez J, Barreiro-Meiro I. Malignant colorectal obstruction treated by means of self-expanding metallic stents: Effectiveness before surgery and in palliation. Radiology. 2000. 216:492–497.2. Mainar A, Ariza MADG, Tejero E, et al. Acute colorectal obstruction treatment with self-expandable metallic stents before scheduled surgery: results of a multicenter study. Radiology. 1999. 210:65–69.3. De Gregorio MA, Mainar A, Tejero E, et al. Acute colorectal obstruction: stent placement for palliative treatment: results of a multicenter study. Radiology. 1998. 209:117–120.4. Saida Y, Sumiyama Y, Narao J, Takase M. Stent endoprosthesis for obstructive colorectal cancers. Dis Colon Rectum. 1996. 39:552–555.5. Loggie BW. Surgical concept in the treatment of colorectal cancer. Semin Roentgenol. 1996. 31:111–117.6. Richards F, Richards CP. Colorectal cancer: etiologic and clinical aspects. Semin Roentgenol. 1996. 31:103–110.7. Choo IW, Do YS, Suh SW, et al. Malignant colorectal obstruction: treatment with a flexible covered stent. Radiology. 1998. 206:415–421.8. Binkert CA, Ledermann H, Jost R, Saurenmann P, Decurtins M, Zollikofer CL. Acute colonic obstruction: clinical aspects and cost-effectiveness of preoperative and palliative treatment with self-expanding metallic stents: a preliminary report. Radiology. 1998. 206:199–204.9. Canon C, Baron TH, Morgan DE, Dean PA, Koehler RE. Treatment of colonic obstruction with expandable metal stents: radiologic features. AJR. 1997. 168:199–205.10. Spinelli R, Fante MD, Mancini A. Self-expanding mesh stent for endoscopic palliation of rectal obstructing tumors: a preliminary report. Surg Endosc. 1992. 6:72–74.11. Rey JF, Romanczyk T, Greff M. Metal stent palliation of rectal carcinoma: a preliminary report on 12 patients. Endoscopy. 1995. 27:501–504.12. Mainar A, Tejero E, Maynar M, Ferral H, Castaneda-Zuniga W. Colorectal obstruction: Treatment with metallic stents. Radiology. 1996. 198:761–764.13. Grunshaw ND, Ball CS. Palliative treatment of an enterorectal fistula with a covered metallic stent. Cardiovasc Intervent Radiol. 2001. 24:438–440.14. Song HY, Lee DH, Seo TS, et al. Retrievable covered nitinol stents: experiences in 108 patients with malignant esophageal strictures. J Vasc Interv Radiol. 2002. 13:285–293.15. Tsunoda S, Shimada Y, Watanabe G, Nakau M, Imamura M. Covered metallic stent treatment of a patient with spontaneous rupture of the esophagus. Dis Esophagus. 2001. 14:254–257.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Colon stenting as a bridge to surgery in obstructive colorectal cancer management
- Combined Treatment with Metallic Stent Placement and Radiotherapy in Malignant Biliary Obstruction
- Fluoroscopic Stent Placement as a Bridge to Surgery for Malignant Colorectal Obstruction: Short- and Long-Term Outcomes
- A Case of Sigmoidorectal Intussusception after Self-Expandable Colonic Stent Placement
- Metal Stent Placement in the Afferent Loop Obstructed by Peritoneal Metastases—Experience of Five Cases
