Thymic Epithelial Tumors Classified According to a Newly Established WHO Scheme: CT and MR Findings
- Affiliations
-
- 1Department of Diagnostic Pathology, Department of Medicine Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. melon2@samsung.co.kr
- 2Department of Radiology and Center for Imaging Science, Department of Medicine Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Thoracic Surgery, Department of Medicine Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Pulmonary and Critical Care Medicine, Department of Medicine Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 754042
- DOI: http://doi.org/10.3348/kjr.2003.4.1.46
Abstract
- Thymic epithelial tumor is a distinctive pathologic entity exhibiting variable histologic features and heterogeneous oncologic behavior. Among the various classification systems, that of the World Health Organization has been adopted because of good correlation between histologic appearance and oncologic behavior. Radiologically, a smooth contour and round shape are most suggestive of a type-A tumor, whereas an irregular contour most strongly suggests type C. Pleural seeding is rare in type-A and AB tumors; calcification is suggestive of type B. Type-C tumors are significantly larger and more commonly associated with lymphadenopathy than type B3. At T2-weighted MR imaging, lobular internal architecture is more prominent in types B1, B2, and B3 tumors than in others. However, imaging findings among the various types overlap to some extent, and the ability of imaging studies to differentiate types AB, B1, B2, and B3 is limited.
Keyword
Figure
-

Fig. 1 Histopathologic demonstration of World Health Organization classification of thymic epithelial tumors (original magnification, ×200; hematoxylin-eosin staining). A. Type A. The tumor consists of haphazardly distributed spindly epithelial tumor cells (arrows). There are few intermingled lymphocytes (arrowheads). B. Type AB. The tumor has two lobular components: a discrete type-A lobule (asterisk) and a sharply juxtaposed type-B lobule (star). The former lobule comprises spindly cells with few lymphocytes, while the latter consists of ovoid epithelial cells admixed with numerous lymphocytes. In other cases, these two lobular components can be intricately admixed. C. Type B1. The tumor consists mostly of a dense population of lymphocytes (mostly immature T cells) (arrows), and some epithelial tumor cells with large nuclei of pale chromatin and small nucleoli (arrowheads). In this tumor, lymphocytes are more abundant than in other thymic epithelial tumors. D. Type B2. The tumor comprises a of nest of epithelial cells (arrowheads). Lymphocytes (arrows) are less abundant than in type B1. E. Type B3. The tumor is composed predominantly of polygonal epithelial cells with nuclear atypia (arrows) and some prominent nucleoli (arrowhead). Note that the nuclei of this type are not uniform and bland. F. Type C. The tumor consists of a nest of squamous cell carcinoma cells (arrows) with severe nuclear atypia and mitotic figures.

Fig. 2 Type-A thymoma in a 51-year-old woman. A. Enhanced 7.0-mm-collimation CT scan obtained at the level of the azygos arch demonstrates homogeneous enhancement. B. Gross pathologic specimen shows that within a pyramid-shaped bilobal thymus, a thymoma (arrow) is present. C. Photomicrograph (original magnification, × 1; hematoxylin-eosin staining) shows that the tumor is completely surrounded by a fibrous capsule (arrows), which is not infiltrated by tumor cells.

Fig. 3 Type-AB thymoma in a 46-year-old-man. A. Enhanced 7.0-mm-collimation CT scan obtained at the level of the azygos arch reveals the presence of a round mass in the right anterior mediastinum. B. T1-weighted (TR/TE, 723/9) MR image obtained at a similar level to A depicts an iso-intense mass. C. Gd-enhanced T1-weighted MR image demonstrates strong tumoral enhancement. D. T2-weighted (TR/TE, 5700/89) MR image shows a mass lesion with slightly higher signal intensity than muscle.
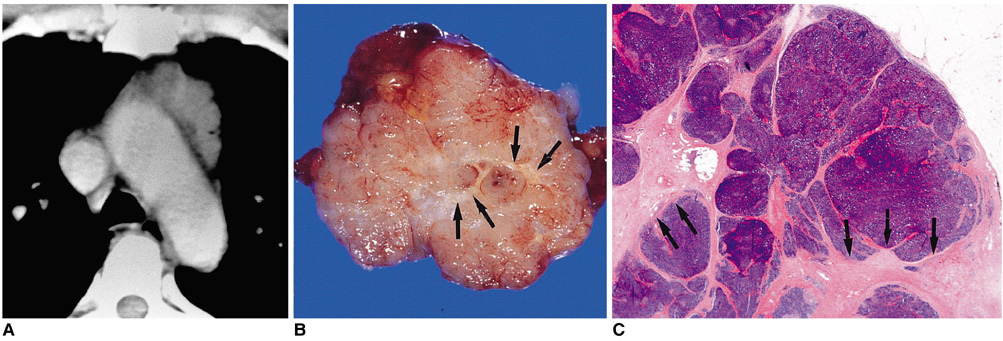
Fig. 4 Type-B1 thymoma in a 48-year-old-man. A. Enhanced 10-mm-collimation CT scan obtained at the level of the aortic arch depicts a well-enhanced homogeneous lobulated mass in the left anterior mediastinum. B. Gross pathologic specimen reveals the presence of well-formed lobules separated by dense fibrous septa (arrows). C. Photomicrograph (original magnification, × 1; hematoxylin-eosin staining) depicts lobulated internal architecture separated by dense fibrous septa (arrows).

Fig. 5 Type-B2 thymoma in a 35-year-old woman. A. Enhanced 10-mm-collimation CT scan obtained at the level of the right interlobar pulmonary artery shows that in the anterior mediastinum, a slightly attenuated heterogeneous mass is present. B. CT scan (10-mm collimation) obtained at the level of the suprahepatic inferior vena cava depicts a pleural mass lesion (arrows) with low attenuation. C. T1-weighted MR image obtained at a similar level to A shows a mass lesion with high-signal intensity. D. T2-weighted image depicts a slightly heterogeneous high-signal lesion. E. Photomicrograph (original magnification, × 1; hematoxylin-eosin staining) shows an invasive tumor bud (arrowheads) penetrating the capsule where there is no fibrous sleeve.
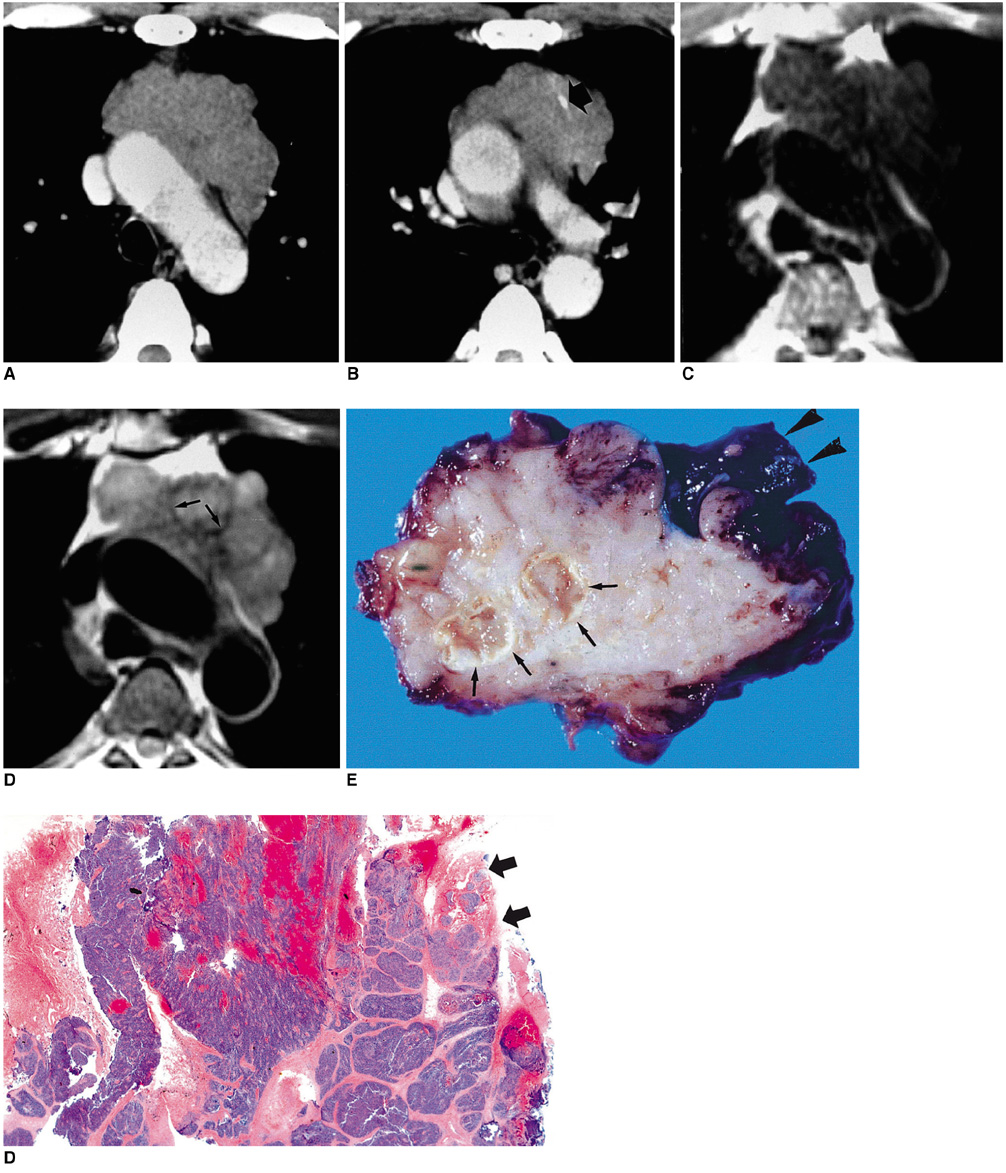
Fig. 6 Type-B3 thymoma in a 50-year-old man with chest pain. A, B. Enhanced 7.0-mm-collimation CT scans obtained at the levels of the aortic arch (A) and main bronchi (B) depict a partly lobulated and irregularly-marginated mass in the anterior mediastinum. There is invasion of mediastinal fat and adjacent lung. Note the presence of nodular calcification (arrow) within the mass lesion depicted in A. C. T1-weighted MR image obtained at the level of the aortic arch reveals the presence of a mass lesion with slightly high signal intensity. D. T2-weighted MR image depicts a lesion of higher signal intensity, broadly attached to the aorta. Note the lobulated internal architecture, separated by low-signal intensity septa (arrows). E. Gross specimen shows pericardial, pleural, aortic, and lung parenchymal involvement (arrowheads). At the cut surface, partially lobulated internal architecture is noted, with thick fibrous septa (arrows). F. Photomicrograph (original magnification, × 1; hematoxylin-eosin staining) discloses no intact capsule (arrows), with lobules of polygonal epithelial cells showing mild nuclear atypia.
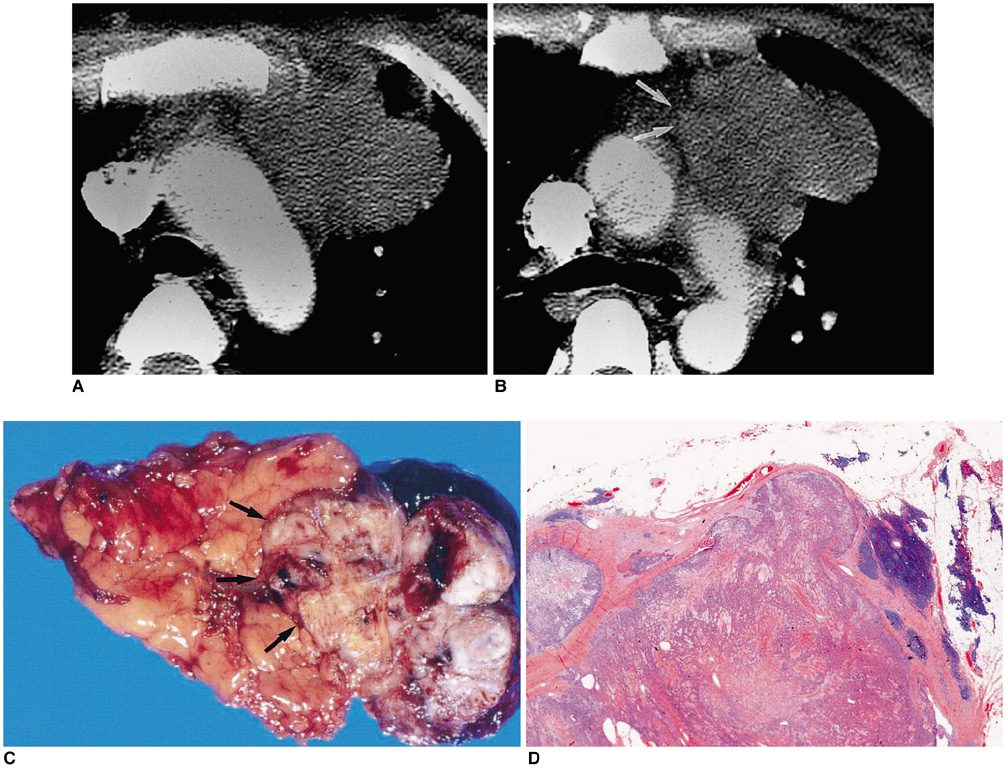
Fig. 7 Type-C thymic carcinoma in a 30-year-old woman with chest pain. A, B. Enhanced 7.0-mm-collimation CT scans obtained at the levels of the aortic arch (A) and main bronchi (B) show a heterogeneously enhancing mass with irregular contour. Also note that the tumor has invaded mediastinal fat (arrows) and the left upper lobe. C. Gross pathologic specimen demonstrates the invasion of mediastinal fal (arrows) by an irregular mass. D. Photomicrograph (original magnification, × 1; hematoxylin-eosin staining) depicts a mass with jigsaw puzzle-like lobules separated by dense fibrous septa. It proved to be type-C thymic carcinoma, with keratinizing squamous cell carcinoma as the main component.

Fig. 8 Type-C thymic carcinoma in a 53-year-old man with chest pain. A. Enhanced 7.0-mm-collimation CT scan obtained at the level of the left innominate vein shows that the anterior mediastinum contains a heterogeneously enhancing irregular mass. Also note nodular pleural thickening (arrowheads) in both hemithoraces, representing pleural seeding. B. Lung window image obtained at the level of the bronchus intermedius demonstrates the presence of small nodules (arrowheads) along major and minor fissures. Also note the presence of pulmonary nodules in the right upper lobe (arrows), representing hematogeneous metastasis.
Reference
-
1. Shimosato Y, Mukai K. Tumors of the mediastinum. Atlas of tumor pathology. 1997. Washington, DC: Armed Forces Institute of Pathology;3rd series, fascicle 21.2. Rosai J, Sobin LH. Histological typing of tumors of the thymus. International histological classification of tumours. 1999. 2nd ed. New York: Springer.3. Tomiyama N, Müller NL, Ellis SJ, et al. Invasive and non-invasive thymoma: distinctive CT features. J Comput Assist Tomogr. 2001. 25:388–393.4. Tomiyama N, Johkoh T, Mihara N, et al. Using the World Health Organization classification of thymic epithelial neoplasms to describe CT findings. AJR Am J Roentgenol. 2002. 179:881–886.5. Jung KJ, Lee KS, Han J, Kim J, Kim TS, Kim EA. Malignant thymic epithelial tumors: CT-pathologic correlation. AJR Am J Roentgenol. 2001. 176:433–439.6. Suster S, Moran CA. Thymoma, atypical thymoma, and thymic carcinoma: A novel conceptual approach to the classification of thymic epithelial neoplasms. Am J Clin Pathol. 1999. 111:826–833.7. Müller-Hermelink HK, Marino M, Palestro G. Pathology of thymic epithelial tumors. Curr Top Pathol. 1986. 75:207–268.8. Okumura M, Miyoshi S, Fujii Y, et al. Clinical and functional significance of WHO classification of human thymic epithelial neoplasms. A study of 146 consecutive tumors. Am J Surg Pathol. 2001. 25:103–110.9. Okumura M, Ohta M, Tateyama H, et al. The World Health Organization histologic classification system reflects the oncological behavior of thymoma: a clinical study of 273 patients. Cancer. 2002. 94:624–632.10. Do YS, Im J-G, Lee BH, et al. CT findings in malignant tumors of thymic epithelium. J Comput Assist Tomogr. 1995. 19:192–197.11. Herold CJ, Zerhouni EA. Higgins CB, Hricak H, Helms CA, editors. The mediastinum and lungs. Magnetic resonance imaging of the body. 1992. 2nd ed. New York: Raven Press.12. Molina PL, Siegel MJ, Glazer HS. Thymic masses on MR imaging. AJR Am J Roentgenol. 1990. 155:495–500.13. Ikezoe J, Takeuchi N, Johkoh T, et al. MRI of anterior mediastinal tumors. Radiat Med. 1992. 10:176–183.14. Sakai F, Sone S, Kiyono K, et al. MR imaging of thymoma: radiologic-pathologic correlation. AJR Am J Roentgenol. 1992. 158:751–756.15. Kushihashi T, Fujisawa H, Munechika H. Magnetic resonance imaging of thymic epithelial tumors. Crit Rev Diagn Imaging. 1996. 37:191–259.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Immunoexpression of Ki-67, Bcl-2, p53, and Tyrosine Kinase Receptors in Thymic Epithelial Tumors; Their Correlation with the WHO Histologic Subtypes and the Prognostic Value
- (18)F-FDG PET/CT is Useful for Pretreatment Assessment of the Histopathologic Type of Thymic Epithelial Tumors
- Anterior Mediastinal Tumor
- Thymic Carcinoma Presenting Two Independent Nodules: Case Report
- Expression of bcl-2 , p53 Protein and Aggressiveness in Thymic Epithelial Tumor
