The role of arthroscopic triangular fibrocartilage complex repair in a case of bilateral Galeazzi fracture-dislocation
- Affiliations
-
- 1Department of Orthopaedic Surgery, Nowon Eulji Medical Center, Eulji University, Seoul, Korea
- 2Department of Orthopaedic Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea
- 3Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2553171
- DOI: http://doi.org/10.12790/ahm.23.0049
Abstract
- This report presents the case of a 23-year-old man with bilateral distal one-third radial shaft fractures and associated distal radioulnar joint disruption, known as Galeazzi fractures, resulting from a fall from a kickboard. After open reduction and plate internal fixation for both radial shafts, the radioulnar joints remained unstable on both sides. We performed arthroscopic repair of the triangular fibrocartilage complex on the left side and used a short arm splint to immobilize the right side. At the 6-month postoperative follow-up, the patient reported mild stiffness in the left wrist, although both sides showed a full range of motion and distal radioulnar joint stability. In conclusion, when achieving anatomic reduction and stable fixation of the radial shaft in a Galeazzi fracture, favorable results can be achieved without additional surgical treatment, even if the distal radioulnar joint is unstable during surgery.
Figure
-
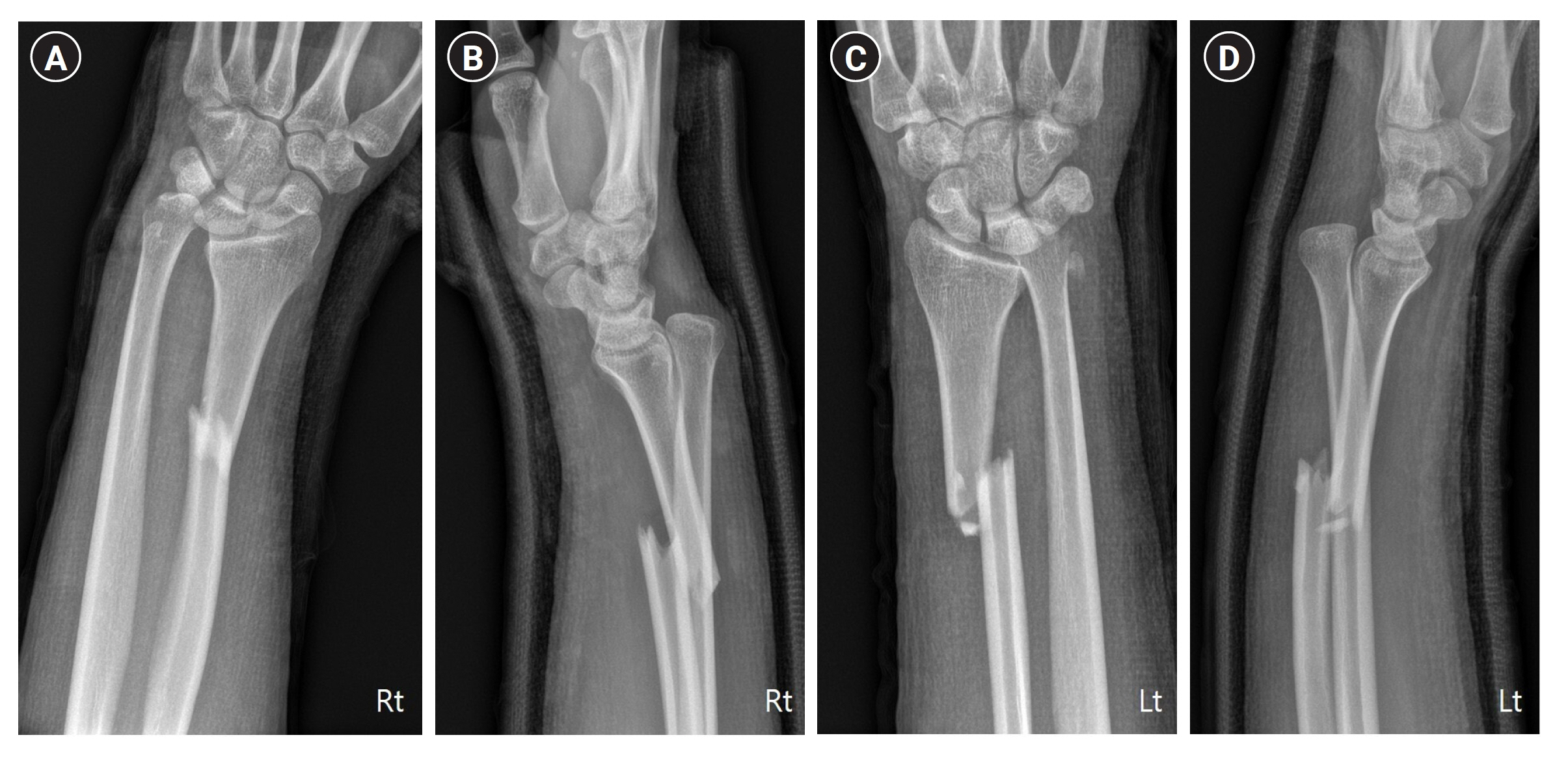
Fig. 1. Preoperative anteroposterior (A) and lateral (B) radiographs of the right wrists demonstrating a Galeazzi fracture-dislocation. On the left side, an almost identical injury pattern was present (C, D). Both radial fractures were located 9 to 10 cm proximal from the joint, and the ulnar head was dislocated dorsally.

Fig. 2. After fixation of the radius fractures, intraoperative stress tests were performed (A, B). Dorsal subluxation of the ulnar head was found in the full pronation position (A).

Fig. 3. On the left side, we performed arthroscopic triangular fibrocartilage complex repair using a bone tunnel. Torn triangular fibrocartilage complex was found (A). We made a bone tunnel (B) and repaired the triangular fibrocartilage complex (C, D).
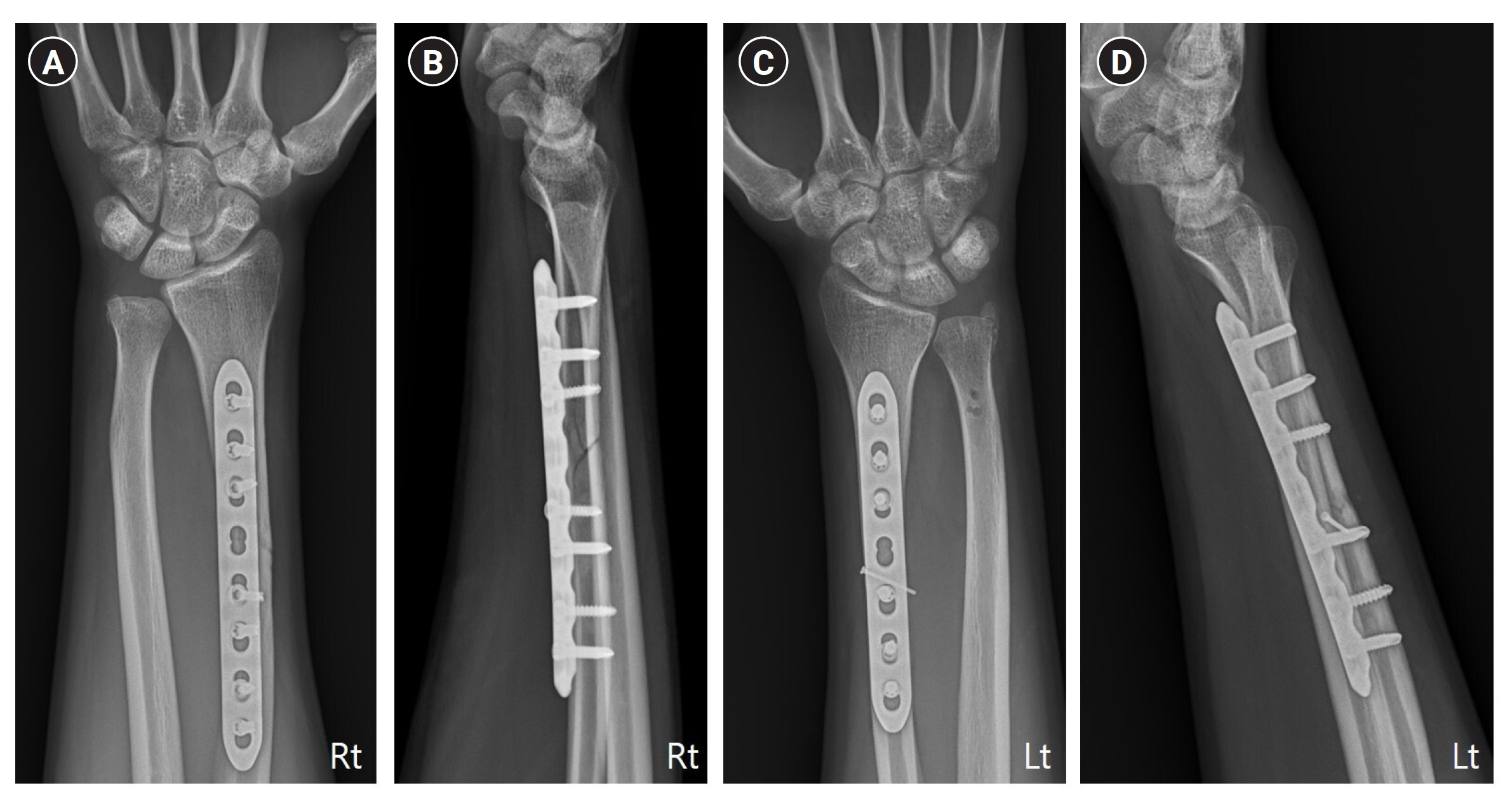
Fig. 4. At a 10-week postoperative follow-up visit, plain anteroposterior (A, C) and lateral (B, D) radiographs presented sound union without distal radioulnar instability.

Fig. 5. The range of motion of both wrists at postoperative 10 weeks.
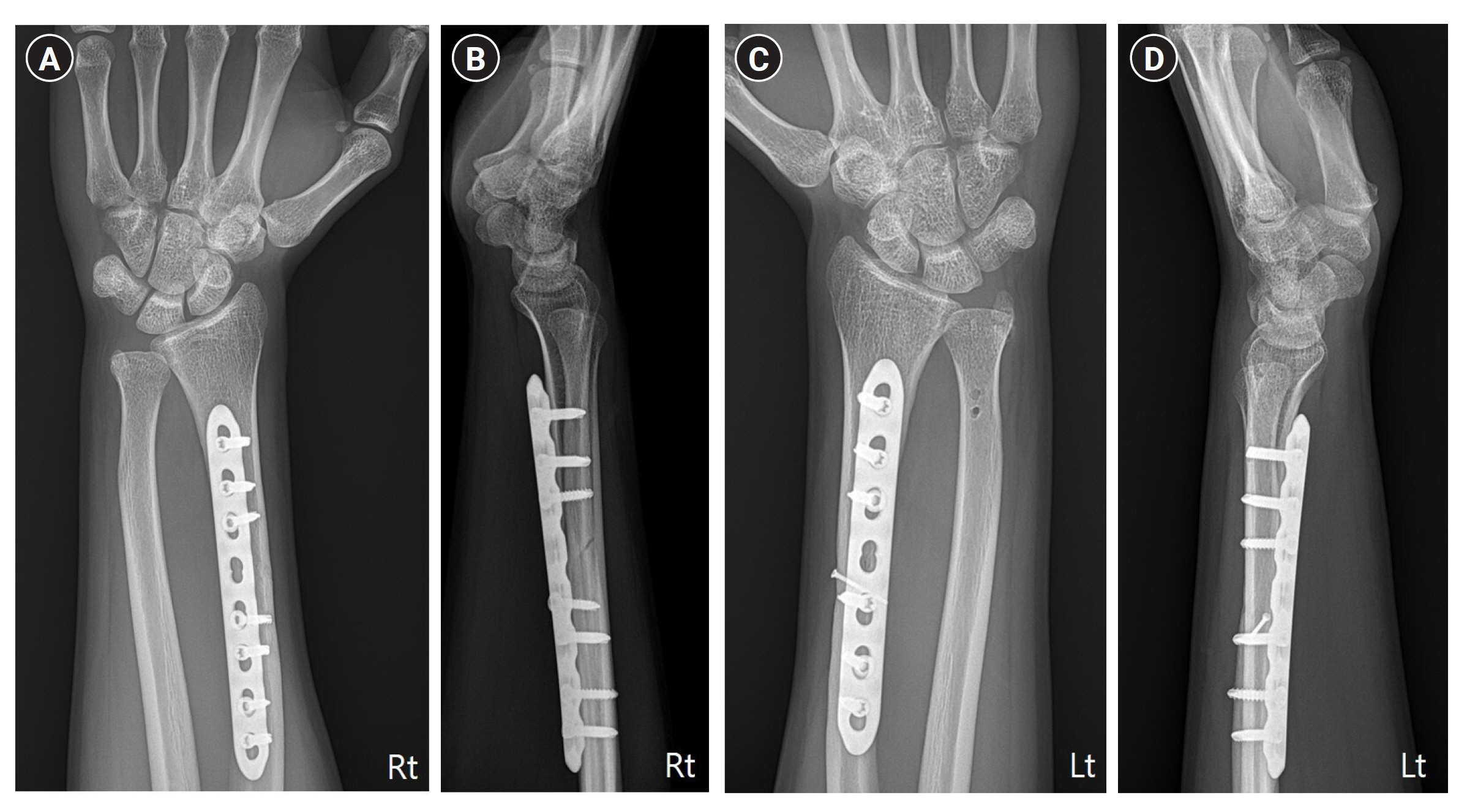
Fig. 6. Plain radiographs at a 1-year postoperative follow-up visit show bony union with a reduced distal radioulnar joint. Anteroposterior and lateral views of the right (A, B) and the left (C, D) wrists were shown.
Reference
-
References
1. Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg Am. 2010; 35:1870–7.
Article2. Atesok KI, Jupiter JB, Weiss AP. Galeazzi fracture. J Am Acad Orthop Surg. 2011; 19:623–33.
Article3. Sivakumaran D, Pathinathan K, Madushanger SR, Gunawardena PM, Dimantha WH, Munidasa D. Bilateral symmetrical pronation type of Galeazzi fracture following high-speed motor traffic crash: a case report. Int J Surg Case Rep. 2021; 85:106284.
Article4. Nanno M, Sawaizumi T, Takai S. Case of bilateral Galeazzi fractures associated with dislocation of the right elbow. J Nippon Med Sch. 2011; 78:384–7.
Article5. Panagopoulos A, Solou K, Tatani I, Kouzelis A, Kokkalis Z. A case of bilateral Galeazzi fracture-dislocations. Cureus. 2021; 13:e17491.
Article6. Alajmi T. Galeazzi fracture dislocations: an illustrated review. Cureus. 2020; 12:e9367.
Article7. Chatterjee D. Early rehabilitation in unstable bilateral Galeazzi fracture dislocation: role of transfixing K wires. Saudi J Sport Med. 2014; 14:168–171.
Article8. Garg R, Mudgal C. Galeazzi injuries. Hand Clin. 2020; 36:455–62.
Article9. Komura S, Nonomura H, Satake T, Yokoi T. Bilateral Galeazzi fracture-dislocations: a case report of early rehabilitation. Strategies Trauma Limb Reconstr. 2012; 7:99–104.
Article10. Borens O, Chehab EL, Roberts MM, Helfet DL, Levine DS. Bilateral Galeazzi fracture-dislocations. Am J Orthop (Belle Mead NJ). 2006; 35:369–72.11. Rettig ME, Raskin KB. Galeazzi fracture-dislocation: a new treatment-oriented classification. J Hand Surg Am. 2001; 26:228–35.
Article12. Gwinn DE, O'Toole RV, Eglseder WA. Early motion protocol for select Galeazzi fractures after radial shaft fixation. J Surg Orthop Adv. 2010; 19:104–8.13. Kim JK, Kook SH, Kim YK. Comparison of forearm rotation allowed by different types of upper extremity immobilization. J Bone Joint Surg Am. 2012; 94:455–60.
Article14. Rahman AM, Montero-Lopez N, Hinds RM, Gottschalk M, Melamed E, Capo JT. Assessment of forearm rotational control using 4 upper extremity immobilization constructs. Hand (N Y). 2018; 13:202–8.
Article15. Weber A, Reissner L, Friedl S, Schweizer A. Stability of the distal radioulnar joint with and without activation of forearm muscles. J Hand Surg Eur Vol. 2023; 48:762–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Knotless Repair
- Surgical Techniques for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Transosseous Repair
- Arthroscopic Repair of Triangular Fibrocartilage Complex Tear
- Arthroscopic Treatment for Triangular Fibrocartilage Complex Lesion
- Ganglion of the Triangular Fibrocartilage Complex: A Case Report
