Arthroscopic Repair of Triangular Fibrocartilage Complex Tear
- Affiliations
-
- 1Department of Orthopedic Surgery, The Catholic University of Korea, Eunpyeong St. Mary’s Hospital, Seoul, Korea
- KMID: 2505897
- DOI: http://doi.org/10.12790/ahm.20.0026
Abstract
- Triangular fibrocartilage complex (TFCC) is an important structure for stability of distal radioulnar joint (DRUJ) and shock absorption of ulnocarpal joint. Recent studies on anatomy and biomechanics of TFCC have revealed that the deep fiber of distal radioulnar ligament plays a key role in stabilizing the DRUJ. Clinicians should evaluate the presence of the instability of DRUJ or ulnar impaction syndrome. If necessary, combined TFCC foveal repair and ulnar shortening osteotomy should be performed. This article introduces the authors’ preferred procedure of arthroscopic TFCC repair with satisfactory clinical outcomes.
Keyword
Figure
-

Fig. 1. Cross section of the triangular fibrocartilage complex. DRUL, distal radioulnar ligament.
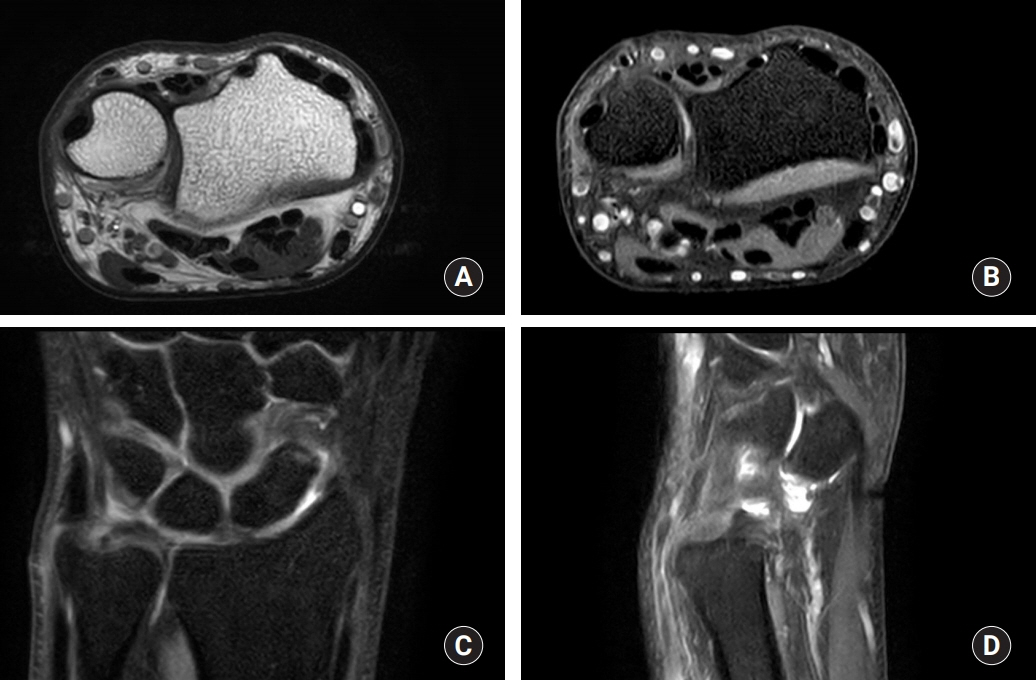
Fig. 2. A 25-year-old male patient sustained left ulnar-sided wrist pain. (A, B) Dorsal subluxation of ulnar head was found in transverse magnetic resonance imaging (MRI) images in T1 and T2. (C) Coronal MRI image showed focal increased signal change in deep fiber of dorsal radioulnar ligament around ulnar fovea. (D) The ulnar head showed dorsal subluxation in sagittal MRI image.

Fig. 3. Trampoline test is an arthroscopic evaluation of tension of triangular fibrocartilage complex.

Fig. 4. The wrist hangs on the traction device with forearm semisupination.
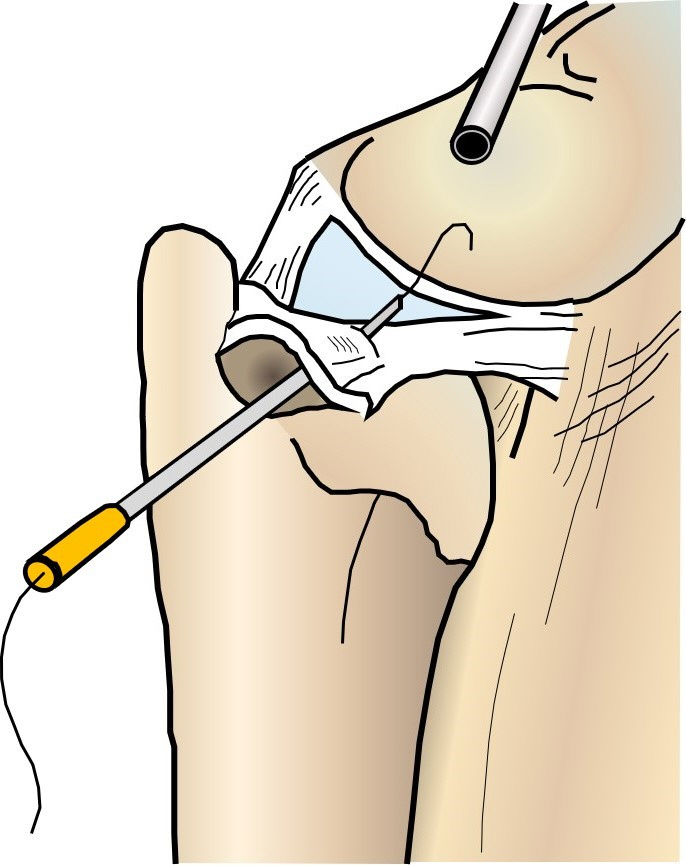
Fig. 5. Schematic drawing shows that 20-gauge needle containing 2-0 Prolene (Ethicon, Somerville, NJ, USA) penetrates the triangular fibrocartilage complex.
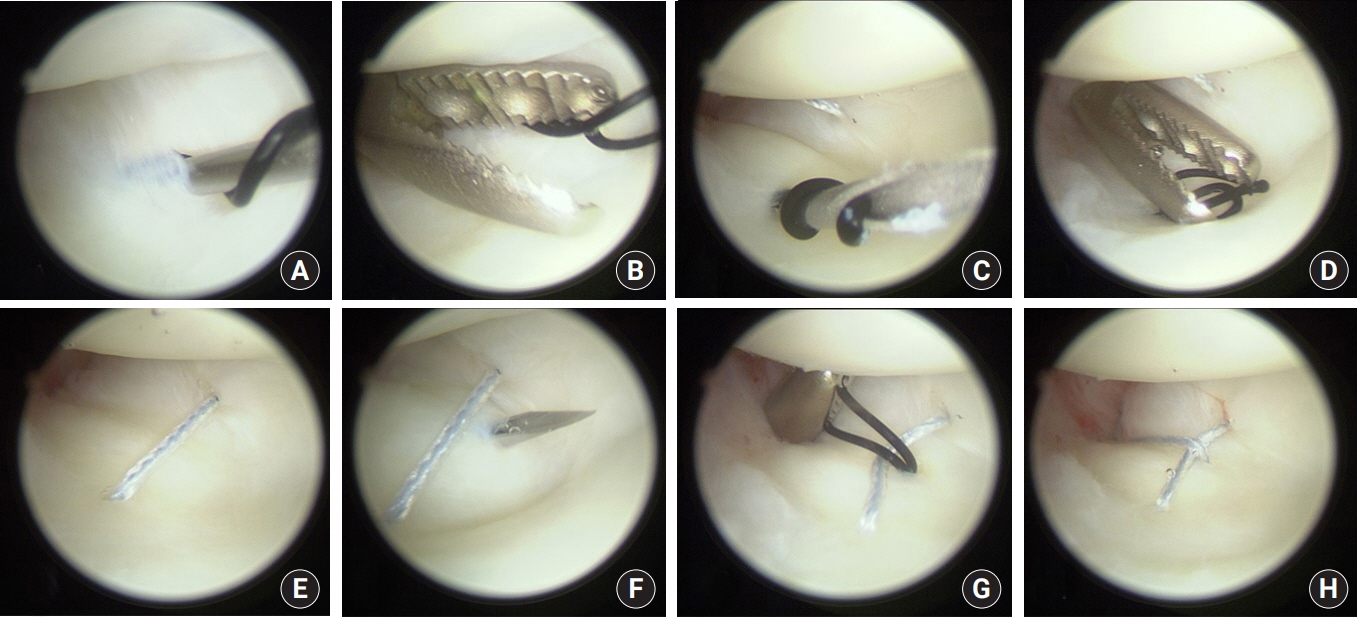
Fig. 6. Arthroscopic images of 30-year-old male patient. (A) With the aid of 20-gauge needle, 2-0 Prolene (Ethicon, Somerville, NJ, USA) passed through the volar part of triangular fibrocartilage complex (TFCC). After taking the intraarticular end of 2-0 Prolene out of the joint, Fiberwire (Arthrex, Naples, FL, USA) and 2-0 Prolene were tied up. (B) Prolene (2-0) substituted for Fiberwire by drawing the untied end of 2-0 Prolene. (C-H) In the same manner, two more stitches on dorsal part and midpoint of TFCC were done to make the Mason-Allen stitch.
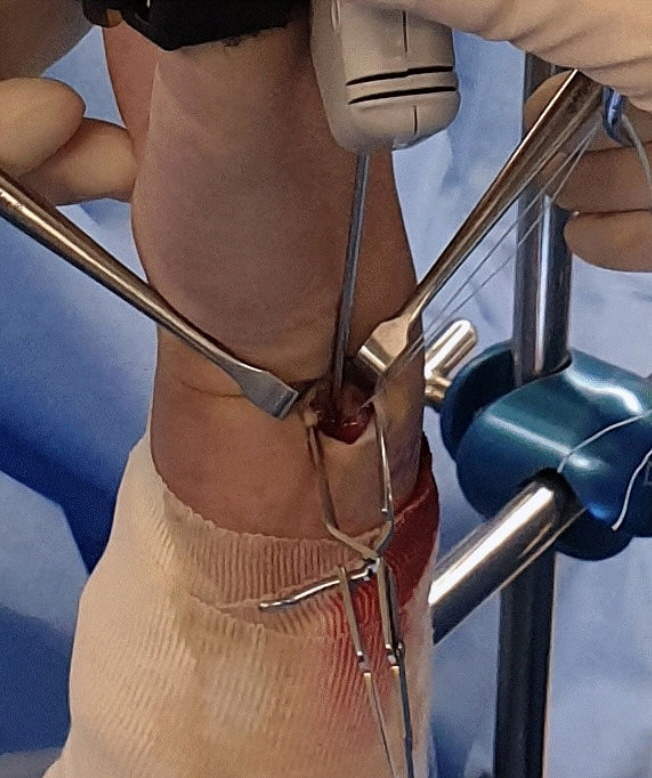
Fig. 7. Suture anchor is placed via 6 ulnar portal. Dorsal branch of ulnar nerve should be protected during the procedure.
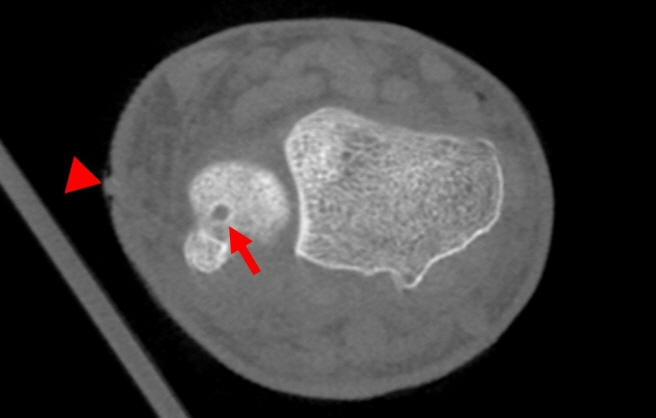
Fig. 8. Postoperative image of computed tomography shows that the anchor (arrow) was inserted in central area of ulnar fovea via 6 ulnar portal (arrowhead).
Reference
-
1. Jang E, Danoff JR, Rajfer RA, Rosenwasser MP. Revision wrist arthroscopy after failed primary arthroscopic treatment. J Wrist Surg. 2014; 3:30–6.
Article2. Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist--anatomy and function. J Hand Surg Am. 1981; 6:153–62.
Article3. Atzei A, Luchetti R. Foveal TFCC tear classification and treatment. Hand Clin. 2011; 27:263–72.
Article4. Tay SC, Tomita K, Berger RA. The “ulnar fovea sign” for defining ulnar wrist pain: an analysis of sensitivity and specificity. J Hand Surg Am. 2007; 32:438–44.
Article5. Petsatodis E, Pilavaki M, Kalogera A, et al. Comparison between conventional MRI and MR arthrography in the diagnosis of triangular fibrocartilage tears and correlation with arthroscopic findings. Injury. 2019; 50:1464–9.
Article6. Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg Am. 1989; 14:594–606.
Article7. Atzei A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur Vol. 2009; 34:582–91.
Article8. Saito T, Sterbenz JM, Chung KC. Chronologic and geographic trends of triangular fibrocartilage complex repair. Hand Clin. 2017; 33:593–605.
Article9. Bednar MS, Arnoczky SP, Weiland AJ. The microvasculature of the triangular fibrocartilage complex: its clinical significance. J Hand Surg Am. 1991; 16:1101–5.
Article10. Estrella EP, Hung LK, Ho PC, Tse WL. Arthroscopic repair of triangular fibrocartilage complex tears. Arthroscopy. 2007; 23:729–37.
Article11. Hagert E, Hagert CG. Understanding stability of the distal radioulnar joint through an understanding of its anatomy. Hand Clin. 2010; 26:459–66.
Article12. Andersson JK, Åhlén M, Andernord D. Open versus arthroscopic repair of the triangular fibrocartilage complex: a systematic review. J Exp Orthop. 2018; 5:6.
Article13. Abe Y, Fujii K, Fujisawa T. Midterm results after open versus arthroscopic transosseous repair for foveal tears of the triangular fibrocartilage complex. J Wrist Surg. 2018; 7:292–7.14. Nakamura T, Nakao Y, Ikegami H, Sato K, Takayama S. Open repair of the ulnar disruption of the triangular fibrocartilage complex with double three- dimensional mattress suturing technique. Tech Hand Up Extrem Surg. 2004; 8:116–23.15. Atzei A, Rizzo A, Luchetti R, Fairplay T. Arthroscopic foveal repair of triangular fibrocartilage complex peripheral lesion with distal radioulnar joint instability. Tech Hand Up Extrem Surg. 2008; 12:226–35.
Article16. Iwasaki N, Minami A. Arthroscopically assisted reattachment of avulsed triangular fibrocartilage complex to the fovea of the ulnar head. J Hand Surg Am. 2009; 34:1323–6.
Article17. Nakamura T, Sato K, Okazaki M, Toyama Y, Ikegami H. Repair of foveal detachment of the triangular fibrocartilage complex: open and arthroscopic transosseous techniques. Hand Clin. 2011; 27:281–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Knotless Repair
- Surgical Techniques for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Transosseous Repair
- Open Repair of Triangular Fibrocartilage Complex Type 1B Tear
- Arthroscopic Repair for Traumatic Peripheral Tear of Triangular Fibrocartilage Complex
- Arthroscopic Treatment for Triangular Fibrocartilage Complex Lesion
