Contributing factors to hand flexor tendon rerupture
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae General Hospital, Gwangmyeong, Korea
- KMID: 2553168
- DOI: http://doi.org/10.12790/ahm.23.0052
Abstract
- Purpose
This retrospective study aimed to identify factors influencing hand flexor tendon rerupture and to develop preventive strategies for patients who have undergone hand flexor tendon repair.
Methods
In total, 287 patients who underwent hand flexor tendon repair between January 2011 and June 2022 were included. Patients with thumb injuries, amputations, bone injuries, extensor tendon injuries, and those with less than 3 months of follow-up were excluded. Patients were divided into rerupture and non-rerupture groups. Events leading to ruptures were also investigated. The two groups were compared according to sex, age, occupation, smoking status, history of diabetes mellitus, injury characteristics, core suture method, and timing of the rehabilitation course.
Results
Of the 287 patients, 19 experienced rerupture (6.6%). The mean time to rerupture was 25.3 days. Reruptures occurred due to unknown causes in nine cases (47.4%), noncompliance with medical recommendations in seven cases (36.8%), and trauma in three cases (15.8%). Among the investigated factors, little finger injury and concurrent flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) ruptures were significantly associated with rerupture. Little difference was noted in the core suture methods and timing of the rehabilitation course between the two groups.
Conclusion
To minimize the risk of rerupture, patients should strictly adhere to medical recommendations and avoid any activities that could cause trauma for at least 1 month after surgery, which is the critical period for tendon remodeling. Patients with little finger injuries as well as concurrent FDS and FDP ruptures require special attention and careful monitoring.
Keyword
Figure
-

Fig. 1. A 16-year-old girl presented with a complete rupture of the flexor digitorum profundus (FDP) tendon due to a cutter knife injury. (A, B) Intraoperative images from the initial repair of the FDP tendon. (C) A 28-day follow-up image showing flexion failure of the distal interphalangeal joint after throwing a book. (D, E) Intraoperative images from the re-repair of the FDP tendon. (F) An 8-month follow-up image after reoperation showing a full range of active flexion motion.

Fig. 2. A 62-year-old man presented with a complete rupture of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendon due to an injury from broken glass. (A, B) Intraoperative images from the initial repair of the FDS and FDP tendons. (C) A 36-day follow-up image showing a limited range of active flexion motion after grabbing a cellphone. (D, E) Intraoperative images from the re-repair of the FDP tendon, with the intact FDS tendon. (F) A 10-month follow-up image after reoperation showing improvement in the range of active flexion motion.
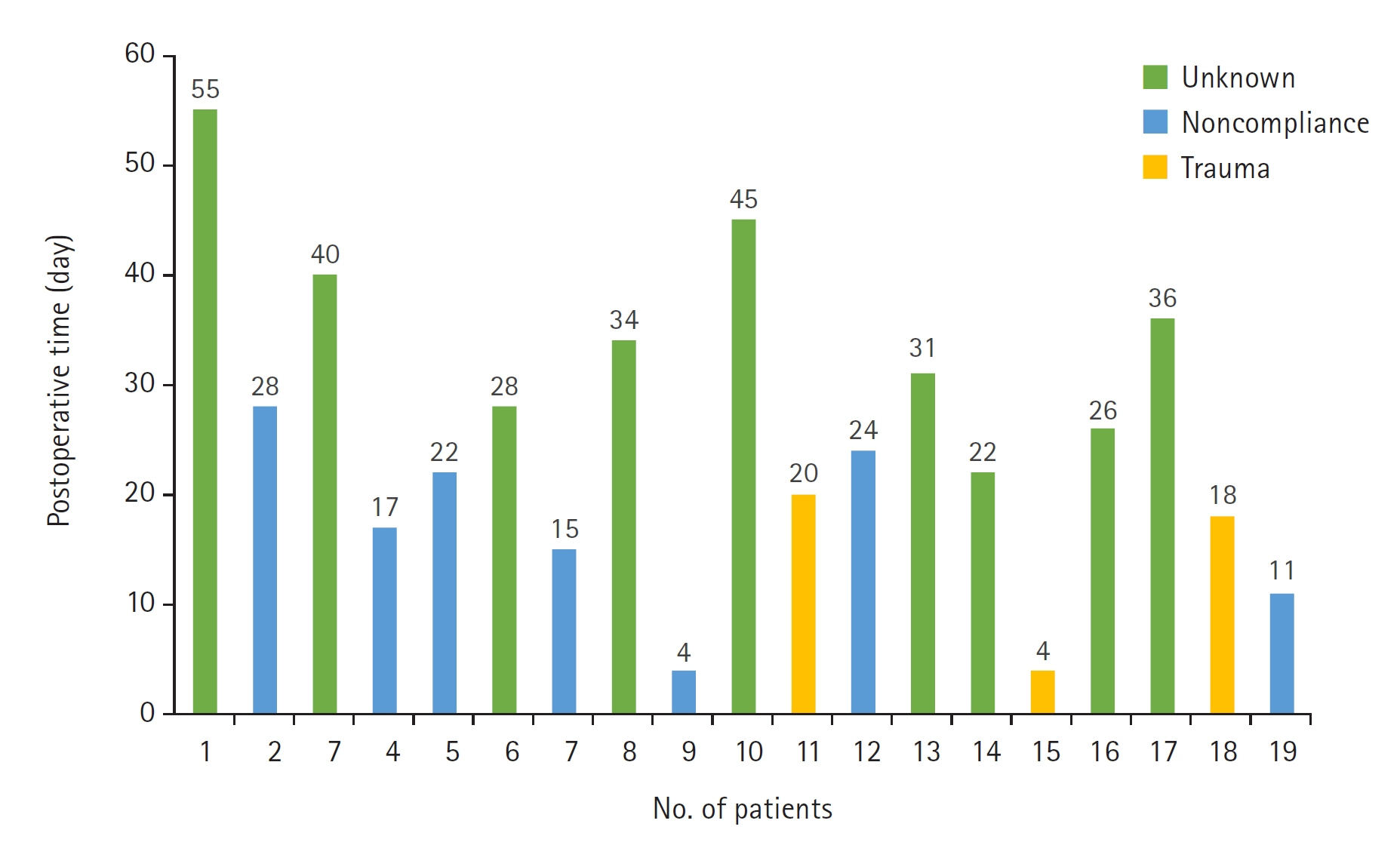
Fig. 3. Distribution of rerupture days for each patient by cause.
Reference
-
References
1. Dy CJ, Daluiski A, Do HT, Hernandez-Soria A, Marx R, Lyman S. The epidemiology of reoperation after flexor tendon repair. J Hand Surg Am. 2012; 37:919–24.
Article2. Dy CJ, Hernandez-Soria A, Ma Y, Roberts TR, Daluiski A. Complications after flexor tendon repair: a systematic review and meta-analysis. J Hand Surg Am. 2012; 37:543–51.
Article3. Ibrahim MS, Khan MA, Rostom M, Platt A. Rupture rate following primary flexor tendon repair of the hand with potential contributing risk factors. Surg Technol Int. 2014; 24:363–7.4. Harris SB, Harris D, Foster AJ, Elliot D. The aetiology of acute rupture of flexor tendon repairs in zones 1 and 2 of the fingers during early mobilization. J Hand Surg Br. 1999; 24:275–80.
Article5. Gomez M. The physiology and biochemistry of soft tissue healing. In : Griffin L, editor. Rehabilitation of the injured knee. St. Louis, MO: Mosby;p. 34–44.6. Lin TW, Cardenas L, Soslowsky LJ. Biomechanics of tendon injury and repair. J Biomech. 2004; 37:865–77.
Article7. Rigo IZ, Røkkum M. Predictors of outcome after primary flexor tendon repair in zone 1, 2 and 3. J Hand Surg Eur Vol. 2016; 41:793–801.
Article8. Gault DT. A review of repaired flexor tendons. J Hand Surg Br. 1987; 12:321–5.
Article9. Dowd MB, Figus A, Harris SB, Southgate CM, Foster AJ, Elliot D. The results of immediate re-repair of zone 1 and 2 primary flexor tendon repairs which rupture. J Hand Surg Br. 2006; 31:507–13.
Article10. Elliot D, Giesen T. Primary flexor tendon surgery: the search for a perfect result. Hand Clin. 2013; 29:191–206.11. Orkar KS, Watts C, Iwuagwu FC. A comparative analysis of the outcome of flexor tendon repair in the index and little fingers: does the little finger fare worse? J Hand Surg Eur Vol. 2012; 37:20–6.
Article12. Svingen J, Wiig M, Turesson C, Farnebo S, Arner M. Risk factors for reoperation after flexor tendon repair: a registry study. J Hand Surg Eur Vol. 2022; 47:1071–6.
Article13. Jia Q, Chen D, Guo J, et al. Risk factors associated with tendon adhesions after hand tendon repair. Front Surg. 2023; 10:1121892.
Article14. Wongsiri S, Liawrungrueang W. Biomechanical study of a newly developed continuous double knots technique compared with the 4-strand double-modified Kessler technique for flexor tendon repair. J Exp Orthop. 2021; 8(1):79.
Article15. Berezin PA, Zolotov AS, Volykhin RD, Evdokimova EN, Morozov LI, Lazarev IA. Rozov and Kessler tendon sutures: common properties and differences. Traumatol Orthop Russ. 2022; 28:167–75.
Article16. Lee KC, Lee DC, Kim JS, Ki SH, Roh SY, Yang JW. Loop suture technique for flexor digitorum profundus tendon repair in the insertion site. J Korean Soc Plast Reconstr Surg. 2010; 37:650–8.17. Lee H. Double loop locking suture: a technique of tendon repair for early active mobilization. Part I: Evolution of technique and experimental study. J Hand Surg Am. 1990; 15:945–52.
Article18. Winters SC, Seiler JG 3rd, Woo SL, Gelberman RH. Suture methods for flexor tendon repair: a biomechanical analysis during the first six weeks following repair. Ann Chir Main Memb Super. 1997; 16:229–34.19. Shaharan S, Bage T, Ibrahim N, Diamantopoulos A, Doswell K, Dheansa B. Rupture rates between 2-strand and 4-strand flexor tendon repairs: is less more? Ann Plast Surg. 2020; 84:43–6.
Article20. Dogramaci Y, Kalaci A, Sevinç TT, Esen E, Komurcu M, Yanat AN. Does strand configuration and number of purchase points affect the biomechanical behavior of a tendon repair?: a biomechanical evaluation using different kessler methods of flexor tendon repair. Hand (N Y). 2008; 3:266–70.
Article21. Small JO, Brennen MD, Colville J. Early active mobilisation following flexor tendon repair in zone 2. J Hand Surg Br. 1989; 14:383–91.
Article22. Khor WS, Langer MF, Wong R, Zhou R, Peck F, Wong JK. Improving outcomes in tendon repair: a critical look at the evidence for flexor tendon repair and rehabilitation. Plast Reconstr Surg. 2016; 138:1045e–1058e.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hamate Hook Fracture with Flexor Tendon Ruptures as a Golf Injury
- Flexor Tendon Rupture Secondary to Gouty Infiltration: A Case Report
- Removal of a Movable Foreign Body in the Flexor Tendon Sheath of the Hand: A Case Report
- Hemangioma of the Flexor Digitorum Superficialis Tendon Sheath in the Hand
- Acute Rupture of Flexor Digitorum Profundus Tendon Associated with Distal Radius Fracture: A Case Report
