Efficacy of an assistive guide tube for improved endoscopic access to gastrointestinal lesions: an in vivo study in a porcine model
- Affiliations
-
- 1Department of Gastroenterology, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
- 2Department of Gastroenterology, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
- 3Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Department of Gastroenterology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2551196
- DOI: http://doi.org/10.5946/ce.2022.161
Abstract
- Background/Aims
Guide tube-assisted endoscopy for procedures that require repeated endoscopic access is safer and more effective than conventional endoscopy. However, its effectiveness has not been confirmed in animal studies. We assessed the usefulness of guide tube-assisted endoscopic procedures in an in vivo porcine model.
Methods
Five different guide tube-assisted endoscopic procedures were performed by experienced endoscopists on a pig weighing 32 kg. To evaluate the efficacy of these procedures, we compared the endoscopic approach time when a guide tube was used to that when it was not. Additional endoscopic procedures using a guide tube were performed, including multiple foreign body extractions, multiple polypectomies, and multiple submucosal dissections. To evaluate safety, we compared the insertion force into the proximal esophagus between the guide tube and conventional overtube methods.
Results
Using the endoscopic approach with a guide tube required a shorter average approach time to reach the three target lesions than when using the endoscopic approach without a guide tube (p<0.001). Compared to the conventional overtube method, the guide tube method produced a lower average resistance during insertion into the upper esophagus (p<0.001).
Conclusions
Guide tube-assisted endoscopic procedures are effective and safe for repeated endoscopic access in an in vivo porcine model.
Keyword
Figure
-
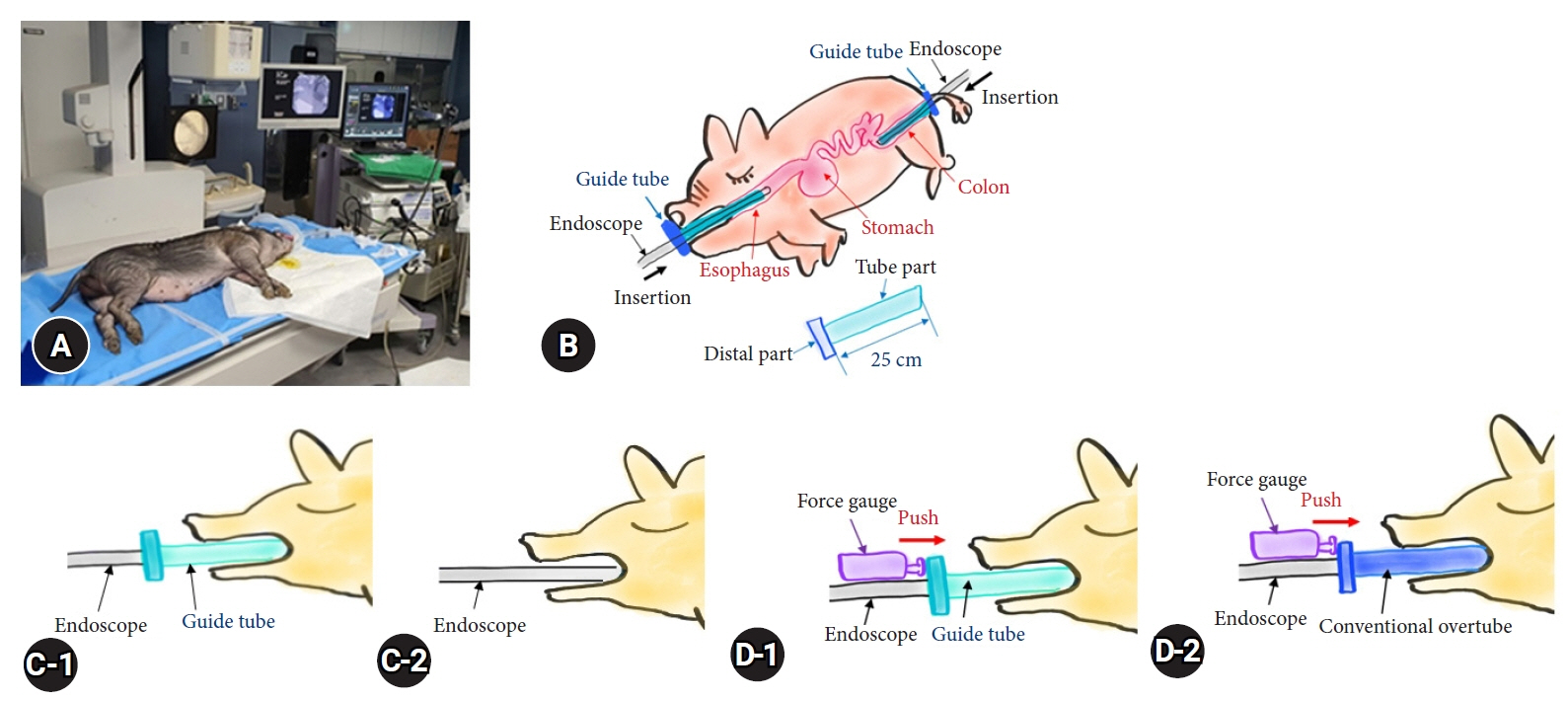
Fig. 1. (A) The in vivo porcine model and the animal room used for endoscopic procedures. (B) Schematic figure of the endoscope, guide tube, and porcine model in this experiment. (C) Measurement of the time for endoscopic approach with the guide tube and that for endoscopic approach without the guide tube. (D) Measurement of insertion force for the guide tube and conventional overtube methods.
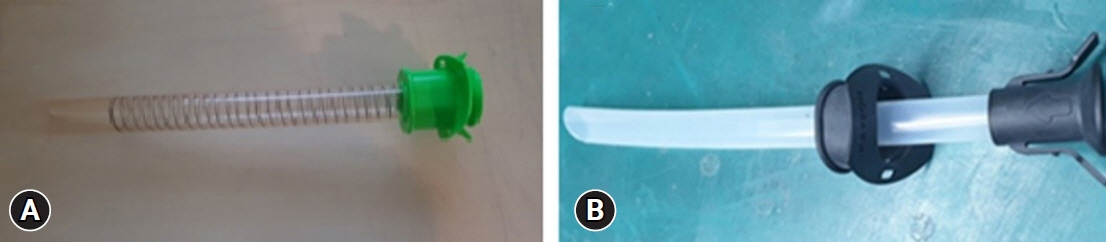
Fig. 2. The two types of overtubes used. (A) A conventional overtube. (B) A guide tube (silicone overtube).

Fig. 3. Endoscopic procedures using the guide tube. (A) Ten pork pieces, measuring 2 cm in diameter, were inserted. (B) An iterative approach into the stomach through the guide tube. (C) A pork piece measuring 2 cm in diameter was removed through the guide tube. (D) Endoscopic mucosal resection of multiple gastric polyps. (E) Endoscopic submucosal dissection of multiple gastric polyps. (F) An iterative approach into the sigmoid colon through the guide tube. (G) Endoscopic mucosal resection of multiple colonic polyps.
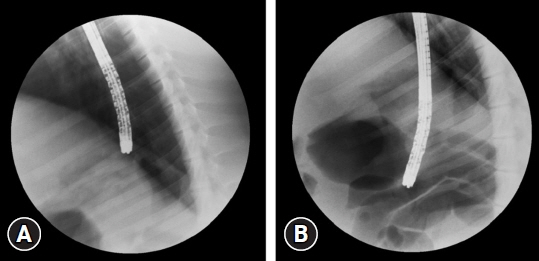
Fig. 4. Abdominal radiographs taken after the guide tube-assisted endoscopic procedures revealed no evidence of tissue perforation. (A) The stomach. (B) The colon.
Reference
-
1. Lee DS, Kim BG, Lee KL, et al. Technical feasibility of a guidetube for various endoscopic procedures in human gastrointestinal simulators. Clin Endosc. 2019; 52:247–251.2. Holderman WH, Etzkorn KP, Patel SA, et al. Endoscopic findings and overtube-related complications associated with esophageal variceal ligation. J Clin Gastroenterol. 1995; 21:91–94.3. Dinning JP, Jaffe PE. Delayed presentation of esophageal perforation as a result of overtube placement. J Clin Gastroenterol. 1997; 24:250–252.4. Levy R, Kaur S, Uzer M. Separation of an overtube from the bite block during band ligation of esophageal varices. Gastrointest Endosc. 1997; 46:66–68.5. Jeffries MA, Scheiman JM. Overtube separation. Gastrointest Endosc. 1998; 47:435–436.6. ASGE Technology Committee, Tierney WM, Adler DG, et al. Overtube use in gastrointestinal endoscopy. Gastrointest Endosc. 2009; 70:828–834.7. Perencevich M, Stoffel EM. A multidisciplinary approach to the diagnosis and management of multiple colorectal polyps. Gastroenterol Hepatol (N Y). 2011; 7:420–423.8. Wang X, Su S, Chen Y, et al. The removal of foreign body ingestion in the upper gastrointestinal tract: a retrospective study of 1,182 adult cases. Ann Transl Med. 2021; 9:502.9. Goldschmiedt M, Haber G, Kandel G, et al. A safety maneuver for placing overtubes during endoscopic variceal ligation. Gastrointest Endosc. 1992; 38:399–400.10. Chen CY, Lin CY, Chang TT, et al. A simple maneuver for placing an overtube during endoscopic variceal ligation. Gastrointest Endosc. 1995; 41:83–84.11. Pai RD, Carr-Locke DL, Thompson CC. Endoscopic evaluation of the defunctionalized stomach by using ShapeLock technology (with video). Gastrointest Endosc. 2007; 66:578–581.12. Raju GS, Pasricha PJ. ShapeLock: a rapid access port for redeployment of a colonoscope into the proximal colon to facilitate multiple polypectomies in a single session. Gastrointest Endosc. 2005; 61:768–770.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Pilot Study of Endoscopic Submucosal Dissection Using an Endoscopic Assistive Robot in a Porcine Stomach Model
- ESD Hands-on Course Using Ex Vivo and In Vivo Models in South Korea
- In vivo porcine training model of laparoscopic common bile duct repair with T-tube insertion under the situation of iatrogenic common bile duct injury
- Observable Laryngopharyngeal Lesions during the Upper Gastrointestinal Endoscopy
- Transvaginal Endoscopic Appendectomy
