Observable Laryngopharyngeal Lesions during the Upper Gastrointestinal Endoscopy
- Affiliations
-
- 1Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea. seenae99@dsmc.or.kr
- KMID: 2048924
- DOI: http://doi.org/10.5946/ce.2013.46.3.224
Abstract
- Regardless of outstanding developments in the endoscopic field, laryngopharyngeal lesions are generally considered as a field of otolaryngology, and thus it is thought that not a lot of gastrointestinal endoscopists commonly take interest in these lesions during the upper gastrointestinal endoscopic examinations. Therefore, here in this thesis, I reviewed the availability of upper gastrointestinal endoscopy in laryngopharyngeal area, normal structures of laryngopharynx, and the lesions that can be observed with the standard upper gastrointestinal endoscopic procedure.
Keyword
Figure
-
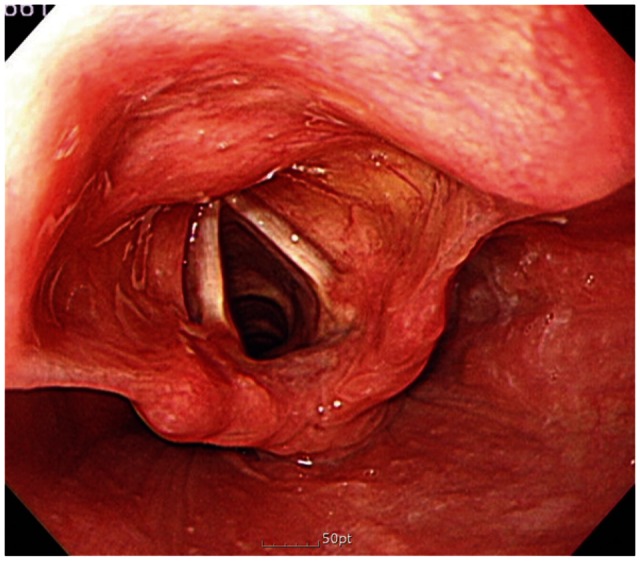
Fig. 1 Normal laryngopharyngeal structure under upper gastrointestinal endoscopic procedure. The vocal cords, insides of the epiglottis, the corniculate cartilage, arytenoids cartilage, and pyriform sinus can be observed.
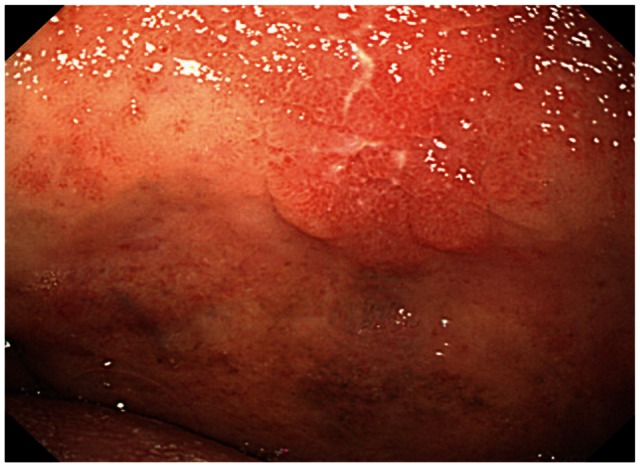
Fig. 2 Soft palate cancer. In a 75-year-old asymptomatic male patient, ill demarcated friable lesion is found on the soft palate.

Fig. 3 Reflux laryngitis. (A) In a 63-year-old male patient who presents severe globus and chronic coughing, diffuse erythema is found in the vocal folds and arytenoids wall. (B) In a 59-year-old male patient who presents globus, severe edema is found in the posterior larynx.
Cited by 1 articles
-
Highlights of the 48th Seminar of Korean Society of Gastrointestinal Endoscopy
Kwang An Kwon, Il Ju Choi, Eun Young Kim, Seok Ho Dong, Ki Baik Hahm
Clin Endosc. 2013;46(3):203-211. doi: 10.5946/ce.2013.46.3.203.
Reference
-
1. Chang DK. Current status of colorectal endoscopic submucosal dissection in Korea. Clin Endosc. 2012; 45:288–289. PMID: 22977820.
Article2. Goh PG, Jeong HY, Kim MJ, et al. Clinical outcomes of endoscopic submucosal dissection for undifferentiated or submucosal invasive early gastric cancer. Clin Endosc. 2011; 44:116–122. PMID: 22741122.
Article3. Kim YS, Cho WY, Cho JY, Jin SY. Successful treatment of early gastric cancer adjacent to a fundal varix by endoscopic submucosal dissection and endoscopic cyanoacrylate therapy. Clin Endosc. 2012; 45:169–173. PMID: 22866260.
Article4. Katsinelos P, Kountouras J, Chatzimavroudis G, et al. Should inspection of the laryngopharyngeal area be part of routine upper gastrointestinal endoscopy? A prospective study. Dig Liver Dis. 2009; 41:283–288. PMID: 18701359.
Article5. Cammarota G, Galli J, Agostino S, et al. Accuracy of laryngeal examination during upper gastrointestinal endoscopy for premalignancy screening: prospective study in patients with and without reflux symptoms. Endoscopy. 2006; 38:376–381. PMID: 16680637.
Article6. Raju GS. Value of screening the laryngopharyngeal area during routine upper gastrointestinal endoscopy. Nat Clin Pract Gastroenterol Hepatol. 2005; 2:22–23. PMID: 16265096.
Article7. Mullhaupt B, Jenny D, Albert S, Schmid S, Fried M. Controlled prospective evaluation of the diagnostic yield of a laryngopharyngeal screening examination during upper gastrointestinal endoscopy. Gut. 2004; 53:1232–1234. PMID: 15306576.
Article8. Yarze JC, Chase MP, Herlihy KJ. Laryngopharyngeal examination: an important but not-so-new role of upper gastrointestinal endoscopy. Ann Intern Med. 2000; 133:314–315. PMID: 10929187.
Article9. Kozarek RA. Evaluation of the larynx, hypopharynx, and nasopharynx at the time of diagnostic upper gastrointestinal endoscopy. Gastrointest Endosc. 1985; 31:271–273. PMID: 4029577.
Article10. Lehman G, Compton M, Meadows J, Elmore M. Screening examination of the larynx and pharynx during upper gastrointestinal panendoscopy. Gastrointest Endosc. 1982; 28:176–178. PMID: 7129039.
Article11. Choi JH, Park JJ, Jee JB, et al. Endoscopic treatment of benign hypopharyngeal tumors. Korean J Gastrointest Endosc. 2005; 31:306–310.12. Matsuo K, Palmer JB. Anatomy and physiology of feeding and swallowing: normal and abnormal. Phys Med Rehabil Clin N Am. 2008; 19:691–707. PMID: 18940636.
Article13. Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006; 101:1900–1920. PMID: 16928254.
Article14. Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA. 2005; 294:1534–1540. PMID: 16189367.
Article15. Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991; 101(4 Pt 2):Suppl 53. 1–78. PMID: 1895864.16. Hickson C, Simpson CB, Falcon R. Laryngeal pseudosulcus as a predictor of laryngopharyngeal reflux. Laryngoscope. 2001; 111:1742–1745. PMID: 11801937.
Article17. Qadeer MA, Swoger J, Milstein C, et al. Correlation between symptoms and laryngeal signs in laryngopharyngeal reflux. Laryngoscope. 2005; 115:1947–1952. PMID: 16319603.
Article18. Hicks DM, Ours TM, Abelson TI, Vaezi MF, Richter JE. The prevalence of hypopharynx findings associated with gastroesophageal reflux in normal volunteers. J Voice. 2002; 16:564–579. PMID: 12512644.
Article19. Branski RC, Bhattacharyya N, Shapiro J. The reliability of the assessment of endoscopic laryngeal findings associated with laryngopharyngeal reflux disease. Laryngoscope. 2002; 112:1019–1024. PMID: 12160267.
Article20. Merati AL, Lim HJ, Ulualp SO, Toohill RJ. Meta-analysis of upper probe measurements in normal subjects and patients with laryngopharyngeal reflux. Ann Otol Rhinol Laryngol. 2005; 114:177–182. PMID: 15825565.
Article21. Noordzij JP, Khidr A, Desper E, Meek RB, Reibel JF, Levine PA. Correlation of pH probe-measured laryngopharyngeal reflux with symptoms and signs of reflux laryngitis. Laryngoscope. 2002; 112:2192–2195. PMID: 12461340.
Article22. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope. 2001; 111:1313–1317. PMID: 11568561.
Article23. Lien HC, Wang CC, Hsu JY, et al. Classical reflux symptoms, hiatus hernia and overweight independently predict pharyngeal acid exposure in patients with suspected reflux laryngitis. Aliment Pharmacol Ther. 2011; 33:89–98. PMID: 21083591.
Article24. Reichel O, Dressel H, Wiederänders K, Issing WJ. Double-blind, placebo-controlled trial with esomeprazole for symptoms and signs associated with laryngopharyngeal reflux. Otolaryngol Head Neck Surg. 2008; 139:414–420. PMID: 18722223.
Article25. Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope. 2001; 111:979–981. PMID: 11404607.
Article26. Scott JC, Jones B, Eisele DW, Ravich WJ. Caustic ingestion injuries of the upper aerodigestive tract. Laryngoscope. 1992; 102:1–8. PMID: 1731151.
Article27. Giannini PJ, Shetty KV. Diagnosis and management of oral candidiasis. Otolaryngol Clin North Am. 2011; 44:231–240. PMID: 21093632.
Article28. Chu EA, Kim YJ. Laryngeal cancer: diagnosis and preoperative work-up. Otolaryngol Clin North Am. 2008; 41:673–695. PMID: 18570953.
Article29. Kim JH, Park JE, Nam JH, et al. A case of synchronous esophageal basaloid squamous carcinoma and cancer of the base of tongue. Korean J Gastrointest Endosc. 2005; 31:383–386.30. Chung KW, Sun HS, Park DH, et al. A case of esophageal cancer with metastasis to the pharynx. Korean J Gastrointest Endosc. 1996; 16:63–67.31. Yoshimura N, Goda K, Tajiri H, et al. Diagnostic utility of narrow-band imaging endoscopy for pharyngeal superficial carcinoma. World J Gastroenterol. 2011; 17:4999–5006. PMID: 22174550.
Article32. Tanaka S, Morita Y, Fujita T, et al. Clinicopathological characteristics of abnormal micro-lesions at the oro-hypopharynx detected by a magnifying narrow band imaging system. Dig Endosc. 2012; 24:100–109. PMID: 22348834.
Article33. Sue RD, Susanto I. Long-term complications of artificial airways. Clin Chest Med. 2003; 24:457–471. PMID: 14535220.
Article34. Jung SW. Two cases of vocal cord paralysis complicated by upper gastrointestinal endoscopy. Korean J Gastrointest Endosc. 2006; 33:32–36.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Introduction to Starting Upper Gastrointestinal Endoscopy: Proper Insertion, Complete Observation, and Appropriate Photographing
- Upper gastrointestinal diseases diagnosed by upper gastrointestinal fiberoptic endoscopy in children
- The Diagnosis of Subepithelial Lesions in the Upper Gastrointestinal Tract
- A Case of Successful Laser Photocoagulation in Gastric Telangiectasias
- Upper Endoscopy in International Digestive Endoscopy Network 2012: Towards Upper End of Quality
