Single-balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy: a technical review
- Affiliations
-
- 1Department of Gastroenterology, Saitama Medical University International Medical Center, Hidaka, Japan
- KMID: 2547891
- DOI: http://doi.org/10.5946/ce.2023.023
Abstract
- Endoscopic retrograde cholangiopancreatography (ERCP) in patients with surgically altered anatomy is technically challenging. For example, scope insertion, selective cannulation, and intended procedures, such as stone extraction or stent placement, can be difficult. Single-balloon enteroscopy (SBE)-assisted ERCP has been used to effectively and safely address these technical issues in clinical practice. However, the small working channel limits its therapeutic potential. To address this shortcoming, a short-type SBE (short SBE) with a working length of 152 cm and a channel of 3.2 mm diameter has recently been introduced. Short SBE facilitates the use of larger accessories to complete certain procedures, such as stone extraction or self-expandable metallic stent placement. Despite the development in the SBE endoscope, various steps have to be overcome to successfully perform such procedure. To improve success, the challenging factors of each procedure must be identified. At the same time, endoscopists need to be mindful of adverse events, such as perforation, which can arise due to adhesions specific to the surgically altered anatomy. This review discussed technical tips regarding SBE-assisted ERCP in patients with surgically altered anatomy to increase success and reduce the risk of adverse events associated with ERCP.
Keyword
Figure
-

Fig. 1. Single-balloon enteroscopy (SBE). (A) A conventional SBE with a 200 cm working length and a 2.8 mm working channel in diameter. (B) A short SBE with a 152 cm working length and a 3.2 mm working channel in diameter.
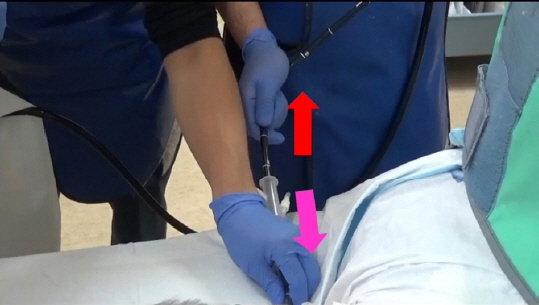
Fig. 2. The way to advance an overtube. Scope itself should be pulled (red arrow) while advancing the overtube (pink arrow).

Fig. 3. Endoscopic findings. (A) A patient with Billroth II gastrectomy. The steep bending part is ordinarily the afferent limb (arrow). (B) A patient with pancreaticoduodenectomy (Child procedure). The steep bending part is ordinarily the afferent limb (arrow). (C) A patient with Roux-en-Y gastrectomy. The disruption of the transverse folds is seen, therefore the slit die of the afferent limb (arrow). (D) A hepaticojejunostomy with Roux-en-Y. There is uncertain whether it is an afferent limb or not.
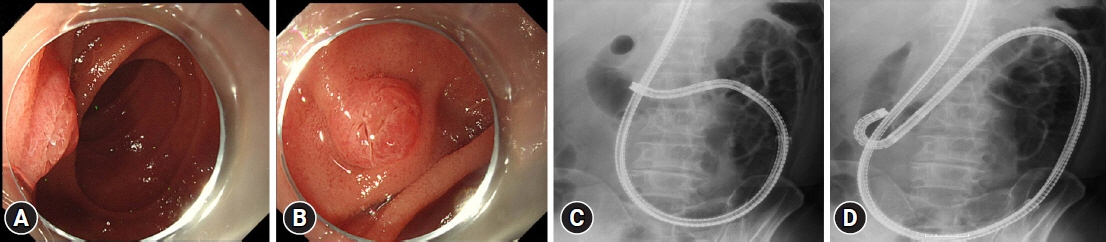
Fig. 4. The retroflex position. (A, C) The papilla is positioned tangentially so it is difficult to perform selective biliary cannulation. (B, D) The scope is advanced while using the up-angle at the inferior duodenal angle, and adjusts to the retroflex position. Consequently, a better view of the papilla can be obtained.

Fig. 5. Selective biliary cannulation using the double-guidewire method. (A, B) Pancreatic duct cannulation is performed and a guidewire is placed in the pancreatic duct. (C, D) As the bile and pancreatic duct are separated well using this method, selective biliary cannulation is achieved.
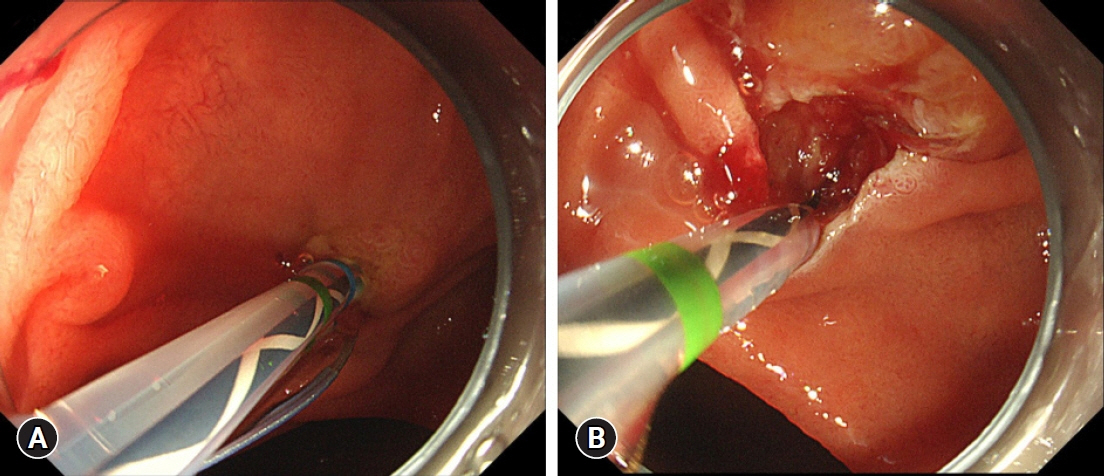
Fig. 6. Endoscopic sphincterotomy (EST) using a dedicated sphincterotomy for patients with surgically altered anatomy. (A) The blade can be easily adjusted towards the 5 o’clock direction, which indicates the bile duct direction in patients with surgically altered anatomy. (B) Successful EST is achieved.
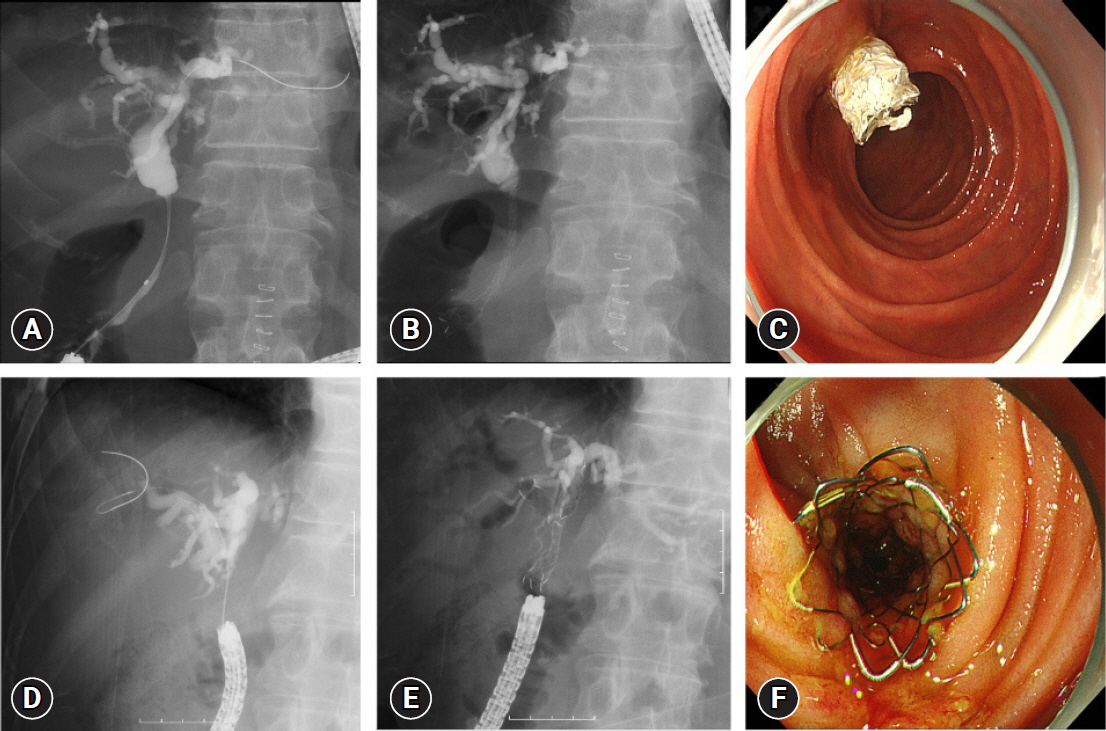
Fig. 7. Self-expandable metallic stent (SEMS) placement in patients with surgically altered anatomy. (A–C) A patient with distal malignant biliary obstruction. Covered SEMS is placed across the papilla. (D–F) A patient with hilar malignant biliary obstruction. Two uncovered SEMS (partial stent in stent method) are placed.
Reference
-
1. Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005; 61:112–125.
Article2. Hintze RE, Adler A, Veltzke W, et al. Endoscopic access to the papilla of Vater for endoscopic retrograde cholangiopancreatography in patients with Billroth II or Roux-en-Y gastrojejunostomy. Endoscopy. 1997; 29:69–73.
Article3. Elton E, Hanson BL, Qaseem T, et al. Diagnostic and therapeutic ERCP using an enteroscope and a pediatric colonoscope in long-limb surgical bypass patients. Gastrointest Endosc. 1998; 47:62–67.
Article4. Wright BE, Cass OW, Freeman ML. ERCP in patients with long-limb Roux-en-Y gastrojejunostomy and intact papilla. Gastrointest Endosc. 2002; 56:225–232.
Article5. Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a nonsurgical steerable double-balloon method. Gastrointest Endosc. 2001; 53:216–220.
Article6. Aabakken L, Bretthauer M, Line PD. Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy. 2007; 39:1068–1071.
Article7. Emmett DS, Mallat DB. Double-balloon ERCP in patients who have undergone Roux-en-Y surgery: a case series. Gastrointest Endosc. 2007; 66:1038–1041.
Article8. Itoi T, Ishii K, Sofuni A, et al. Single-balloon enteroscopy-assisted ERCP in patients with Billroth II gastrectomy or Roux-en-Y anastomosis (with video). Am J Gastroenterol. 2010; 105:93–99.
Article9. Wang AY, Sauer BG, Behm BW, et al. Single-balloon enteroscopy effectively enables diagnostic and therapeutic retrograde cholangiography in patients with surgically altered anatomy. Gastrointest Endosc. 2010; 71:641–649.
Article10. Tanisaka Y, Ryozawa S, Mizuide M, et al. Status of single-balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy: systematic review and meta-analysis on biliary interventions. Dig Endosc. 2021; 33:1034–1044.
Article11. Tanisaka Y, Ryozawa S, Mizuide M, et al. Usefulness of the “newly designed” short-type single-balloon enteroscope for ERCP in patients with Roux-en-Y gastrectomy: a pilot study. Endosc Int Open. 2018; 6:E1417–E1422.
Article12. Tanisaka Y, Mizuide M, Fujita A, et al. Competence development of trainees performing short-type single-balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. J Hepatobiliary Pancreat Sci. 2022; 29:1316–1326.
Article13. Tanisaka Y, Mizuide M, Fujita A, et al. Factors affecting complete stone extraction in the initial procedure in short type single-balloon enteroscopy-assisted endoscopic retrograde cholangiography for patients with Roux-en-Y gastrectomy. Scand J Gastroenterol. 2022; 57:1390–1396.
Article14. Shimatani M, Takaoka M, Ikeura T, et al. Evaluation of endoscopic retrograde cholangiopancreatography using a newly developed short-type single-balloon endoscope in patients with altered gastrointestinal anatomy. Dig Endosc. 2014; 26 Suppl 2:147–155.
Article15. Kawamura T, Uno K, Suzuki A, et al. Clinical usefulness of a short-type, prototype single-balloon enteroscope for endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy: preliminary experiences. Dig Endosc. 2015; 27:82–86.
Article16. Yane K, Katanuma A, Maguchi H, et al. Short-type single-balloon enteroscope-assisted ERCP in postsurgical altered anatomy: potential factors affecting procedural failure. Endoscopy. 2017; 49:69–74.
Article17. Tanisaka Y, Ryozawa S, Mizuide M, et al. Analysis of the factors involved in procedural failure: endoscopic retrograde cholangiopancreatography using a short-type single-balloon enteroscope for patients with surgically altered gastrointestinal anatomy. Dig Endosc. 2019; 31:682–689.
Article18. Tanisaka Y, Ryozawa S, Itoi T, et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy-assisted ERCP for altered anatomy: a multicenter cohort in Japan. Gastrointest Endosc. 2022; 95:310–318.
Article19. Zhu F, Guan Y, Wang J. Efficacy and safety of the rotatable sphincterotome during ERCP in patients with prior Billroth II gastrectomy (with videos). Surg Endosc. 2021; 35:4849–4856.
Article20. Park TY, Bang CS, Choi SH, et al. Forward-viewing endoscope for ERCP in patients with Billroth II gastrectomy: a systematic review and meta-analysis. Surg Endosc. 2018; 32:4598–4613.
Article21. Yano T, Hatanaka H, Yamamoto H, et al. Intraluminal injection of indigo carmine facilitates identification of the afferent limb during double-balloon ERCP. Endoscopy. 2012; 44 Suppl 2 UCTN:E340–E341.
Article22. Iwai T, Kida M, Yamauchi H, et al. Short-type and conventional single-balloon enteroscopes for endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy: single-center experience. Dig Endosc. 2014; 26 Suppl 2:156–163.23. Kanno Y, Ohira T, Kozakai F, et al. Accurate endoscopic identification of the afferent limb at the Y anastomosis using the fold disruption sign after gastric resection with Roux-en-Y reconstruction. Dig Endosc. 2022; 34:238–243.
Article24. Tokuhara M, Shimatani M, Mitsuyama T, et al. Evaluation of complications after endoscopic retrograde cholangiopancreatography using a short type double balloon endoscope in patients with altered gastrointestinal anatomy: a single-center retrospective study of 1,576 procedures. J Gastroenterol Hepatol. 2020; 35:1387–1396.
Article25. Yang MJ, Hwang JC, Yoo BM, et al. Balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography. Korean J Pancreas Biliary Tract. 2021; 26:205–208.
Article26. Ishii K, Itoi T, Tonozuka R, et al. Balloon enteroscopy-assisted ERCP in patients with Roux-en-Y gastrectomy and intact papillae (with videos). Gastrointest Endosc. 2016; 83:377–386.
Article27. Tanisaka Y, Ryozawa S, Mizuide M, et al. Biliary cannulation in patients with Roux-en-Y gastrectomy: an analysis of the factors associated with successful cannulation. Intern Med. 2020; 59:1687–1693.
Article28. Ito K, Horaguchi J, Fujita N, et al. Clinical usefulness of double-guidewire technique for difficult biliary cannulation in endoscopic retrograde cholangiopancreatography. Dig Endosc. 2014; 26:442–449.
Article29. Tanisaka Y, Ryozawa S, Mizuide M, et al. Novel technique using pancreatic duct stent facilitates difficult biliary cannulation in patients with Roux-en-Y anatomy (with video). JGH Open. 2019; 4:296–298.
Article30. Takenaka M, Minaga K, Kamata K, et al. Efficacy of a modified double-guidewire technique using an uneven double lumen cannula (uneven method) in patients with surgically altered gastrointestinal anatomy (with video). Surg Endosc. 2020; 34:1432–1441.
Article31. Sato T. TXI: texture and color enhancement imaging for endoscopic image enhancement. J Healthc Eng. 2021; 2021:5518948.
Article32. Tanisaka Y, Mizuide M, Fujita A, et al. Use of texture and color enhancement imaging to identify the pancreatic duct orifice in a patient with a pancreaticojejunal anastomotic stricture. Endoscopy. 2023; 55(S 01):E88–E89.
Article33. Tanisaka Y, Mizuide M, Fujita A, et al. A novel sphincterotome facilitates endoscopic sphincterotomy in patients with Roux-en-Y gastrectomy. Endoscopy. 2022; 54(S 02):E780–E781.
Article34. Obata T, Tsutsumi K, Kato H, et al. Balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography for the treatment of common bile duct stones in patients with Roux-en-Y gastrectomy: outcomes and factors affecting complete stone extraction. J Clin Med. 2021; 10:3314.
Article35. Iwashita T, Nakai Y, Hara K, et al. Endoscopic ultrasound-guided antegrade treatment of bile duct stone in patients with surgically altered anatomy: a multicenter retrospective cohort study. J Hepatobiliary Pancreat Sci. 2016; 23:227–233.
Article36. Ogura T, Kawai J, Nishiguchi K, et al. Transluminal intrahepatic bile duct stone removal using a novel spiral basket catheter via the endoscopic ultrasound-guided hepaticogastrostomy route (with video). Dig Endosc. 2022; 34:234–237.
Article37. Tanisaka Y, Ryozawa S, Mizuide M, et al. Usefulness of self-expandable metal stents for malignant biliary obstruction using a short-type single-balloon enteroscope in patients with surgically altered anatomy. J Hepatobiliary Pancreat Sci. 2021; 28:272–279.
Article38. Takeda T, Sasaki T, Mie T, et al. The safety and efficacy of self-expandable metallic stent placement for malignant biliary obstruction with surgically altered anatomy. Scand J Gastroenterol. 2021; 56:94–102.
Article39. Kogure H, Sato T, Nakai Y, et al. Endoscopic management of pancreatic diseases in patients with surgically altered anatomy: clinical outcomes of combination of double-balloon endoscopy- and endoscopic ultrasound-guided interventions. Dig Endosc. 2021; 33:441–450.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent advances of endoscopic retrograde cholangiopancreatography in surgically altered anatomy
- Single Balloon Enteroscopy-Guided Endoscopic Retrograde Cholangiopancreatography in Surgically Altered Anatomy: Long vs. Short Type
- Single Balloon Enteroscopy-Assisted Endoscopic Retrograde Cholangiopancreatography in Patients Who Underwent a Gastrectomy with Roux-en-Y Anastomosis: Six Cases from a Single Center
- Endoscopic ultrasound-directed transgastric endoscopic retrograde cholangiopancreatography for patients with Roux-en-Y gastric bypass anatomy: technical overview
- Endoscopic Ultrasound-Guided Pancreatobiliary Endoscopy in Surgically Altered Anatomy
