Successful Simultaneous Treatment of Benign Stricture and Colonic Neoplasm Arising from Colonic Interposition after Esophagectomy: A Case Report
- Kim SH1
- Kim JW1
- Park SY1
- Kim HS1
- Lim CJ1
- Lee GH1
- Lim JW1
- Seo YE1
- Park SY1
- Lee YH1
- Jung YW1
- Kang WR1
- You HS1
- Kim DH
 1
1
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Chonnam National University Hospital and Medical School, Gwangju, Korea
- KMID: 2546516
- DOI: http://doi.org/10.4166/kjg.2023.080
Abstract
- Colonic interposition is the main procedure used in esophageal reconstruction. We report a rare case of simultaneous treatment of an anastomotic site stricture and a neoplasm in the interpositioned colon. A 69-year-old female visited our outpatient clinic with symptoms of progressive dysphagia for 1 year. At the age of 30 years, the patient underwent esophagectomy with retrosternal colonic interposition because of severe esophageal burns after chemical ingestion. Upper gastrointestinal endoscopy revealed stricture at the anastomosis site and a 10-mm flat elevated high-grade dysplasia in the interpositioned colon. First, through-the-scope balloon dilatation was performed for strictures. However, stenosis was observed during the second upper gastrointestinal endoscopy session. Therefore, a second session of through-the-scope balloon dilatation was performed, and simultaneously, endoscopic submucosal dissection was also successfully performed. After 2 months of follow-up, stenosis persisted; consequently, balloon dilatation was performed. No recurrence of neoplasm was confirmed endoscopically. Through-the-scope balloon dilatation of the stricture site and simultaneous endoscopic submucosal dissection of the neoplasm in the interpositioned colon were successfully performed.
Keyword
Figure
-
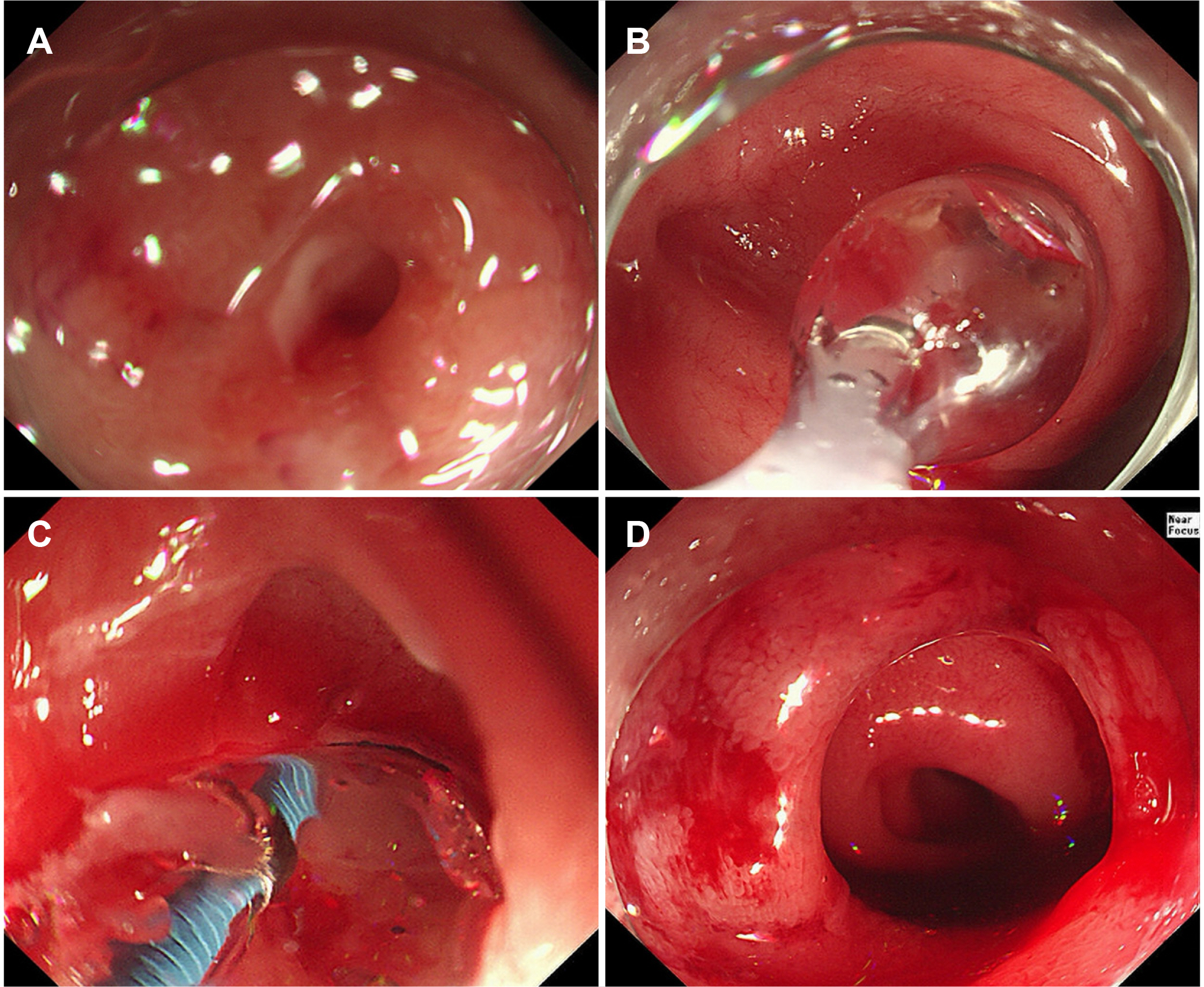
Fig. 1 The first through-the-scope (TTS) balloon dilatation to treat the stenosis. (A) An approximately 18–23 cm site from the upper incisor, which is the proximal anastomotic site, demonstrating luminal narrowing with near total obstruction. (B–D) Treatment with the first TTS balloon dilatation.

Fig. 2 Feature of the detected nodular lesion, treated by endoscopic submucosal dissection (ESD), and pathological examination results. (A, B) An approximately 10-mm nodular lesion was observed at 33 cm from the upper incisor position. (C, D) Performance of ESD. (E, F) Resected tissue. (G, H) Histologic examination of the resected lesion revealed a high-grade dysplasia with R0 resection (hematoxylin and eosin staining; magnification, ×20 and ×100, respectively).
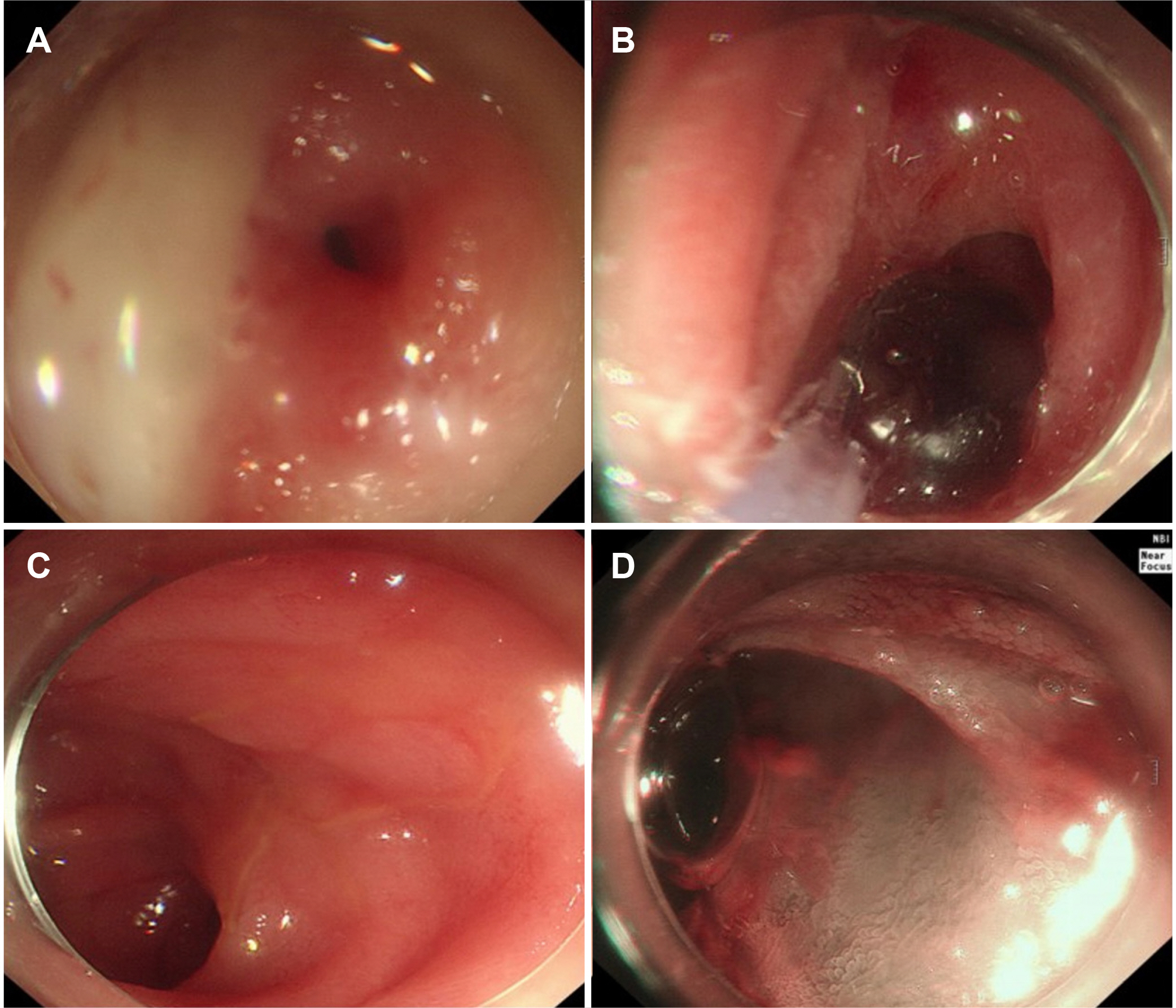
Fig. 3 Through-the-scope (TTS) balloon dilatation was repeated due to re-stenosis, and endoscopic submucosal dissection (ESD) of the site was checked. (A) Follow-up endoscopy that confirmed recurrence of the stenosis. (B) A third TTS balloon dilatation was performed. (C, D) ESD scar lesion was checked. No evidence of recurrence was observed endoscopically.
Reference
-
1. Ng DW, Ching Tan GH, Teo MC. 2016; Malignancy arising in a 41-year-old colonic interposition graft. Asian J Surg. 39:45–47. DOI: 10.1016/j.asjsur.2014.01.002. PMID: 24637188.2. Barbosa B, Santos B, Mesquita I, Marcos M, Nogueira C, Santos J. 2018; Adenocarcinoma arising in a colonic interposition after esophagectomy for benign stricture and review of the literature. J Surg Case Rep. 2018:rjy264. DOI: 10.1093/jscr/rjy264. PMID: 30310649. PMCID: PMC6172699.3. Gallo G, Zwaveling S, Groen H, Van der Zee D, Hulscher J. 2012; Long-gap esophageal atresia: a meta-analysis of jejunal interposition, colon interposition, and gastric pull-up. Eur J Pediatr Surg. 22:420–425. DOI: 10.1055/s-0032-1331459. PMID: 23212741.4. Chiu YC, Hsu CC, Chiu KW, Chuah SK, Changchien CS, Wu KL, et al. 2004; Factors influencing clinical applications of endoscopic balloon dilation for benign esophageal strictures. Endoscopy. 36:595–600. DOI: 10.1055/s-2004-814520. PMID: 15243881.5. van Boeckel PG, Siersema PD. 2015; Refractory esophageal strictures: what to do when dilation fails. Curr Treat Options Gastroenterol. 13:47–58. DOI: 10.1007/s11938-014-0043-6. PMID: 25647687. PMCID: PMC4328110.6. Shersher DD, Hong E, Warren W, Penfield Faber L, Liptay MJ. 2011; Adenocarcinoma in a 40-year-old colonic interposition treated with Ivor Lewis esophagectomy and esophagogastric anastomosis. Ann Thorac Surg. 92:e113–e114. DOI: 10.1016/j.athoracsur.2011.06.025. PMID: 22115265.7. Saleem M, Iqbal A, Ather U, Haider N, Talat N, Hashim I, et al. 2020; 14 Years' experience of esophageal replacement surgeries. Pediatr Surg Int. 36:835–841. DOI: 10.1007/s00383-020-04649-5. PMID: 32236666. PMCID: PMC7223057.8. Bando H, Ikematsu H, Fu KI, Oono Y, Kojima T, Minashi K, et al. 2010; A laterally-spreading tumor in a colonic interposition treated by endoscopic submucosal dissection. World J Gastroenterol. 16:392–394. DOI: 10.3748/wjg.v16.i3.392. PMID: 20082488. PMCID: PMC2807963.9. Ferlitsch M, Moss A, Hassan C, Bhandari P, Dumonceau JM, Paspatis G, et al. 2017; Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 49:270–297. DOI: 10.1055/s-0043-102569. PMID: 28212588.10. Park CH, Yang DH, Kim JW, Kim JH, Kim JH, Min YW, et al. 2020; [Clinical practice guideline for endoscopic resection of early gastrointestinal cancer]. Korean J Gastroenterol. 75:264–291. [Korean]. DOI: 10.4166/kjg.2020.75.5.264. PMID: 32448858.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Jejunal Free Graft for Complicated Corrosive Esophageal Stricture
- A Case of Benign Colonic Stricture Treated by Therapeutic Balloon Dilatation in Ulcerative Colitis
- Esophagectomy for Benign Esophageal Disease
- Two Cases of Robot-Assisted Totally Minimally Invasive Esophagectomy with Colon Interposition for Gastroesophageal Junction Cancer: Surgical Considerations
- Colon Stricture After Ischemia Following a Robot-Assisted Ultra-Low Anterior Resection With Coloanal Anastomosis
