An adolescent female with intentional ingestion of a large amount of metformin requiring extracorporeal membrane oxygenation and continuous renal replacement therapy
- Affiliations
-
- 1Department of Pediatrics, Eastern Virginia Medical School, Norfolk, VA, United States
- 2Department of Critical Care, Children’s Hospital of the King’s Daughters, Norfolk, VA, United States
- 3Nephrology, Children’s Hospital of the King’s Daughters, Norfolk, VA, United States
- KMID: 2546289
- DOI: http://doi.org/10.22470/pemj.2023.00759
Abstract
- Acute overdose of metformin can show potentially fatal lactic acidosis. Management should be directed towards close monitoring of renal function and hemodynamics. Patients may require dialysis or extracorporeal membrane oxygenation in cases of hemodynamic instability. This case presents an adolescent with massive metformin ingestion estimated at 100 g leading to metformin-associated lactic acidosis and subsequent respiratory failure, cardiovascular collapse, and acute kidney injury. The complications were successfully managed with venoarterial extracorporeal membrane oxygenation, continuous renal replacement therapy, and mechanical ventilation.
Keyword
Figure
-
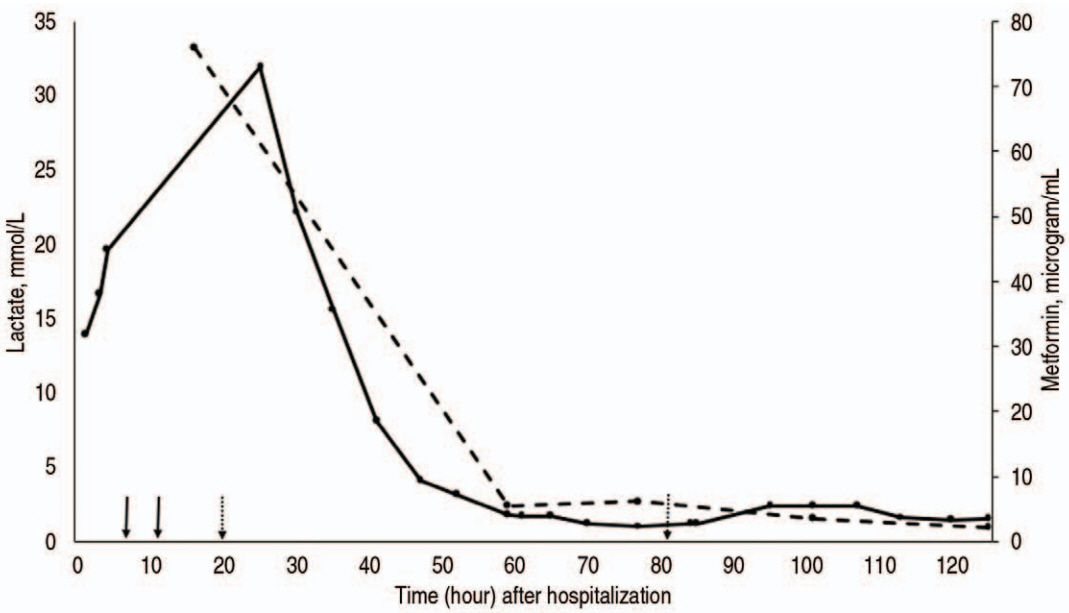
Fig. 1. Trend of serum concentrations of lactate (solid line) and metformin (dashed line) during the hospitalization, with relation to extracorporeal removal techniques (solid arrows: initiation of hemodialysis and transition to continuous renal replacement therapy [from left to right]; dotted arrows: ECMO cannulation and decannulation). Ongoing lactic acidosis and shock prompted transition from hemodialysis (hour 7) to continuous venovenous hemodiafiltration (hour 11) and venoarterial ECMO (cannulation at hour 20, decannulation at hour 81). After the initiation of ECMO, lactate concentration began to downtrend and normalized around 48 hours. Norepinephrine and epinephrine were discontinued at hour 30 and 79, respectively. The peak concentration of lactate was 31.9 mmol/L, which was measured 17 hours after initiation of dialysis and 4 hours after initiation of ECMO. The peak concentration of metformin was 76 μg/mL, which was measured 8 hours after the initiation of dialysis. ECMO: extracorporeal membrane oxygenation.
Reference
-
References
1. Dell’Aglio DM, Perino LJ, Kazzi Z, Abramson J, Schwartz MD, Morgan BW. Acute metformin overdose: examining serum pH, lactate level, and metformin concentrations in survivors versus nonsurvivors: a systematic review of the literature. Ann Emerg Med. 2009; 54:818–23.2. Calello DP, Liu KD, Wiegand TJ, Roberts DM, Lavergne V, Gosselin S, et al. Extracorporeal treatment for metformin poisoning: systematic review and recommendations from the Extracorporeal Treatments in Poisoning Workgroup. Crit Care Med. 2015; 43:1716–30.3. DeFronzo R, Fleming GA, Chen K, Bicsak TA. Metformin-associated lactic acidosis: current perspectives on causes and risk. Metabolism. 2016; 65:20–9.4. Kopec KT, Kowalski MJ. Metformin-associated lactic acidosis (MALA): case files of the Einstein Medical Center Medical Toxicology Fellowship. J Med Toxicol. 2013; 9:61–6.5. Wang GS, Hoyte C. Review of biguanide (metformin) toxicity. J Intensive Care Med. 2019; 34:863–76.6. Al-Abri SA, Hayashi S, Thoren KL, Olson KR. Metformin overdose-induced hypoglycemia in the absence of other antidiabetic drugs. Clin Toxicol. 2013; 51:444–7.7. Kinoshita H, Yanai M, Ariyoshi K, Ando M, Tamura R. A patient with metformin-associated lactic acidosis successfully treated with continuous renal replacement therapy: a case report. J Med Case Rep. 2019; 13:371.8. Cole JB, Olives TD, Ulici A, Litell JM, Bangh SA, Arens AM, et al. Extracorporeal membrane oxygenation for poisonings reported to U.S. Poison Centers from 2000 to 2018: an analysis of the National Poison Data System. Crit Care Med. 2020; 48:1111–9.9. Blumenberg A, Benabbas R, Sinert R, Jeng A, Wiener SW. Do Patients die with or from metformin-associated lactic acidosis (MALA)? Systematic review and meta-analysis of pH and lactate as predictors of mortality in MALA. J Med Toxicol. 2020; 16:222–9.10. Akoglu H, Akan B, Piskinpasa S, Karaca O, Dede F, Erdem D, et al. Metformin-associated lactic acidosis treated with prolonged hemodialysis. Am J Emerg Med. 2011; 29:575.e3–5.11. Spiller HA, Weber JA, Winter ML, Klein-Schwartz W, Hofman M, Gorman SE, et al. Multicenter case series of pediatric metformin ingestion. Ann Pharmacother. 2000; 34:1385–8.12. Spiller HA, Quadrani DA. Toxic effects from metformin exposure. Ann Pharmacother. 2004; 38:776–80.13. Lacher M, Hermanns-Clausen M, Haeffner K, Brandis M, Pohl M. Severe metformin intoxication with lactic acidosis in an adolescent. Eur J Pediatr. 2005; 164:362–5.14. Bebarta VS, Pead J, Varney SM. Lacticemia after acute overdose of metformin in an adolescent managed without intravenous sodium bicarbonate or extracorporeal therapy. Pediatr Emerg Care. 2015; 31:589–90.15. Harvey B, Hickman C, Hinson G, Ralph T, Mayer A. Severe lactic acidosis complicating metformin overdose successfully treated with high-volume venovenous hemofiltration and aggressive alkalinization. Pediatr Crit Care Med. 2005; 6:598–601.16. Gunay E, Kalkan Z, Selim Ay M, Yuksel E, Berekatoglu N, Yaman M. Successful dialysis treatment of metformin associated lactic acidosis, report of two cases. Iran J Kidney Dis. 2020; 14:160–4.17. Chen T, Zhu C, Liu B. Extracorporeal membrane oxygenation with continuous renal replacement therapy to treat metformin-associated lactic acidosis: a case report. Medicine (Baltimore). 2020; 99:e20990.18. Chang A, Rai A, Zavin A, Rizwan M. Veno arterial extracorporeal membrane oxygenation in a case of metformin induced metabolic acidosis. Chest. 2020; 158(4 Suppl):A786.19. Wang GS, Levitan R, Wiegand TJ, Lowry J, Schult RF, Yin S, et al. Extracorporeal membrane oxygenation (ECMO) for severe toxicological exposures: review of the Toxicology Investigators Consortium (ToxIC). J Med Toxicol. 2016; 12:95–9.20. Ives Tallman C, Zhang Y, Black N, Lynch K, Fayed M, Armenian P. Refractory vasodilatory shock secondary to metformin overdose supported with VA ECMO. Toxicol Rep. 2021; 9:64–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extracorporeal Membrane Oxygenation and Continuous Renal Replacement Therapy for Treatment of Calcium Channel Blockers, Angiotensin II Receptor Blockers, and Metformin Overdose
- Simultaneous Extracorporeal Membrane Oxygenation, Renal Replacement Therapy, and Plasma Exchange for Thrombocytopenia-Associated Multiple Organ Failure
- Management of Cyanide Intoxication with Extracorporeal Membrane Oxygenation and Continuous Renal Replacement Therapy
- Outcomes of patients with COVID-19 requiring extracorporeal membrane oxygenation and continuous renal replacement therapy in the United States
- Continuous Renal Replacement Therapy in Infants and Neonates
