Ultrasonic Osteotome Assisted Posterior Endoscopic Cervical Foraminotomy in the Treatment of Cervical Spondylotic Radiculopathy Due to Osseous Foraminal Stenosis
- Affiliations
-
- 1Department of Neurosurgery, Minhang Hospital, Fudan University, Shanghai, China
- 2Department of Neurosurgery, Zhongshan Hospital, Fudan University, Shanghai, China
- KMID: 2543534
- DOI: http://doi.org/10.3340/jkns.2022.0233
Abstract
Objective
: To investigate the efficacy and safety of the posterior endoscopic cervical foraminotomy (PECF) using ultrasonic osteotome for the treatment of cervical osseous foraminal stenosis,focusing on introduction of the advantages of ultrasonic osteotome in partial pediculectomy and ventral osteophyte resection in PECF.
Methods
: Nineteen patients with cervical osseous foraminal stenosis who underwent PECF using ultrasonic osteotome in our institution between April 2018 and April 2021 were enrolled in this study. All the patients were followed up more than 12 months. The patients’ medical data, as well as pre- and postoperative radiologic findings were thoroughly investigated. The visual analogue score (VAS), Japanese Orthopaedic Association (JOA) score, cervical dysfunction index (Neck disability index, NDI), and modified MacNab criteria were used to assess the surgical efficacy.
Results
: All the patients were successfully treated with PECF using ultrasonic osteotome. The pre- and postoperative VAS, NDI, and JOA scores were significantly improved (p<0.05). According to the modified MacNab criteria, 17 patients were assessed as “excellent”, two patients were assessed as “good” at the last follow-up. There was no dura tear, nerve root damage, incision infection, neck deformity, or other complications.
Conclusion
: Adequate nerve root decompression can be accomplished successfully with the help of ultrasonic osteotome in PECF, which has the advantage of reducing the probability of damage to the nerve root and dura mater, in addition to the original merits of endoscopic surgery.
Keyword
Figure
-
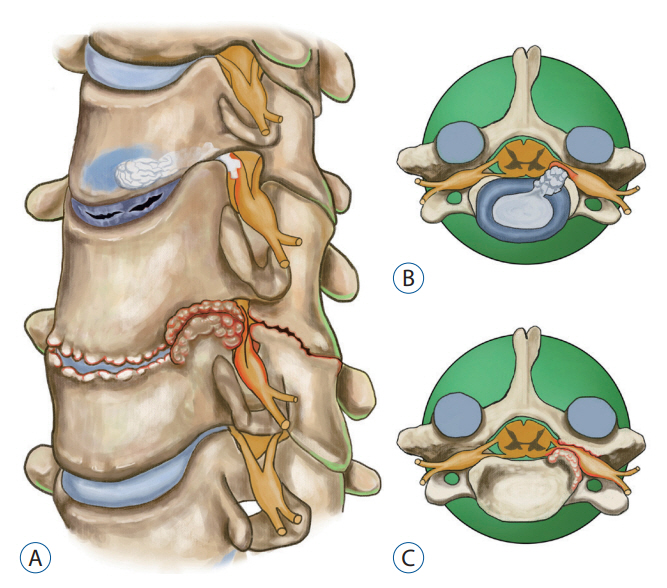
Fig. 1. Illustration showing the causes of cervical spondylotic radiculopathy. A : Indicating disc collapse, disc herniation and osteophyte hyperplasia with osseous foraminal stenosis respectively. B : Cervical disc herniation extruding the nerve root. C : Cervical nerve root compressed by osseous foraminal stenosis.

Fig. 2. A : Illustration showing the operating room layout. The host machine of the ultrasonic osteotome is next to endoscopic workstation. The operator is using endoscopic ultrasonic osteotome compatible with endoscopic working channel in PECF. B : Illustration showing ultrasonic osteotome (XD860A SMTP Technology, Beijing, China) profile, including diameter, length, and shape.
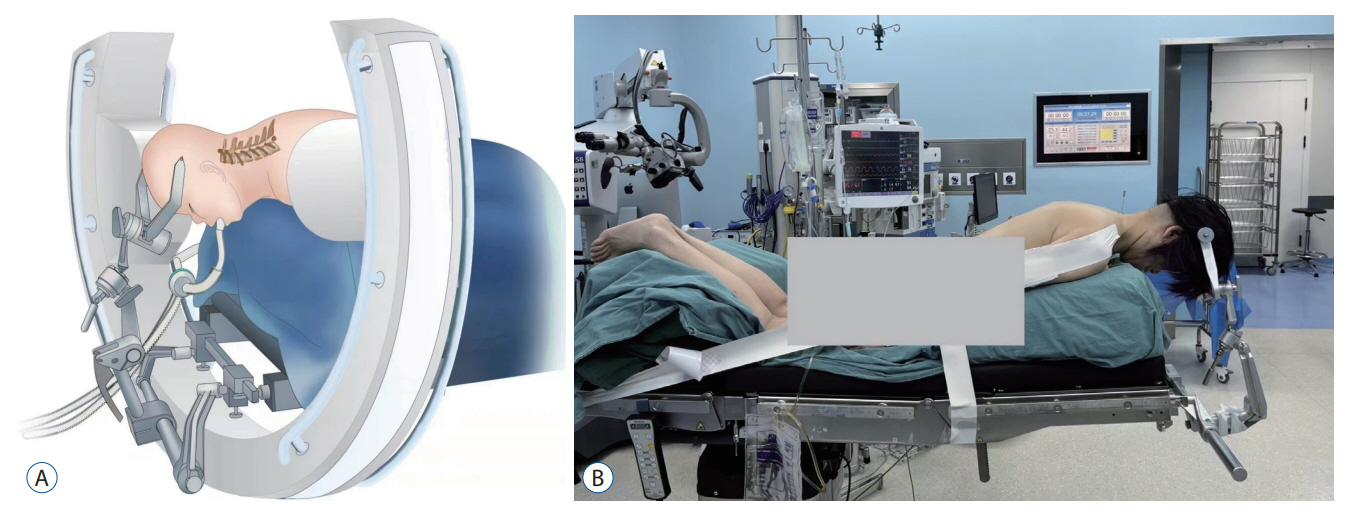
Fig. 3. A : Schematic diagram showing the position of the patient under movable C-arm fluoroscope. B : The patient was placed in the prone position with head fixed in the Mayfield clamp under general anesthesia.

Fig. 4. A : Lateral fluoroscopy showing the spinal needle was introduced to touch the bone, which is C5-6 facet joint. B : Anteroposterior fluoroscopy showing the tip of needle was located in projection of pedicle. C and D : The position of the working cannula was controlled radiologically in anteroposterior and lateral position; (C) lateral view and (D) anteroposterior view.

Fig. 5. Intraoperative endoscopic view of representative case 1. A : The “V-point” structure was identified. B : The C7 pedicle was identified which located inferior of the left C7 nerve root. The pedicle was close and at same level to root and dura. Using high-speed drill here was dangerous. C : Endoscopic ultrasound osteotome was used to perform partial pediculectomy. D : The ventral osteophyte was exposed after partial pediculectomy (white arrow represented hyperplasia of Luschka joint, black arrow represented the space which the original position of the pedicle located and now be removed). E : The ventral osteophyte was handled by ultrasonic osteotome without significant neural retraction. F : The C7 nerve root was fully decompressed and freed.

Fig. 6. Illustrations showing the application of endoscopic ultrasonic osteotome in posterior endoscopic cervical foraminotomy. A : Showing the application of endoscopic ultrasonic osteotome compatible with endoscopic working channel and the “key hole”. B-D : Illustrations showing the top view of application of ultrasonic osteotome. B : Endoscopic ultrasound osteotome was used to perform partial pediculectomy to enlarge the operation space. C : The ventral osteophyte could be handled by ultrasonic osteotome. D : The affected nerve root was 360° decompressed safely. E and F : Illustrations showing the side view of application of ultrasonic osteotome. E : After resection of medial half of the facet joint, endoscopic ultrasound osteotome was used to perform partial pediculectomy to enlarge the operation space. F : The ventral osteophyte could be handled by ultrasonic osteotome.

Fig. 7. Intraoperative endoscopic view of representative case 2. A : Left C4 nerve root was exposed which located within narrowed C3-C4 intervertebral foramen. The distance between the upper and lower pedicle was significantly reduced. B : Endoscopic ultrasound osteotome was used to perform partial C3 pediculectomy (at the same level with C4 nerve root). C : Endoscopic ultrasound osteotome was used to perform partial C4 pediculectomy and partial vertebral body resection (this location is below the level of the nerve root). D : The left C4 nerve root was fully decompressed and freed.

Fig. 8. During the follow-up time, the neck and arm VAS scores, JOA scores and the NDI improved significantly. VAS : visual analogue score, preop : preoperative, F/U : follow-up, JOA : Japanese Orthopaedic Association, NDI : Neck disability index.

Fig. 9. Clinical results according to the modifield MacNab criteria.

Fig. 10. The preoperative and postoperative imaging data of representative case 1. A, C, and G : Preoperative magnetic resonance imaging (MRI) and computed tomography (CT) studies showed osseous foraminal stenosis at the left side of the C6/7 level. B, D, and H : Postoperative MRI and CT image showed removal of the ventral osseous and decompression of the nerve root (arrow in D and H represented the intervertebral foramen has been enlarged). E : Preoperative CT reconstruction scan showed severe hyperplasia of Luschka joint with narrowing of the left C6-C7 foramen. F : Postoperative sagittal CT reconstruction showed the enlargement of C6-C7 intervertebral foramen (arrow) with partial pediculectomy and ventral osseous removal. I : The 3D reconstruction showed the keyhole (arrow) decompression range, which preserved the facet joint more than 50%.

Fig. 11. The preoperative and postoperative imaging data of representative case 2. A, C and G : Preoperative magnetic resonance imaging (MRI) and computed tomography (CT) reconstruction images showing osseous foraminal stenosis at the left side of the C3/4 level due to cage subside and insufficient decompression. B, D, and H : Postoperative MRI and CT image showed removal of the osseous and decompression of the nerve root (arrow in D and H represented the intervertebral foramen has been enlarged). E : Preoperative sagittal CT reconstruction scan showing intervertebral height was lost and the distance between the upper and lower pedicle was significantly reduced with narrowing of the left C3-C4 foramen. F : Postoperative sagittal CT reconstruction shows the left C3-C4 intervertebral foramen (arrow) was enlarged with partial pediculectomy and ventral osteophyte removal. I : The position of the working cannula was controlled radiologically in the lateral position. J : The 3D reconstruction showed the keyhole (arrow) decompression range, which preserved the facet joint more than 50%.

Fig. 12. Illustration showing the pedicle and the nerve root are in the same level. It is dangerous when the high-speed rotating bit bounce or slip, resulting involvement of nerve elements. A : So, the nerve root and dural sac should be pushed away. Even so, the risk remains. Moreover, excessive pushing will also cause damage to the nerves. B : On the contrary, endoscopic ultrasound osteotome has advantages in this respect. It can help us securely resect part of the pedicle without worrying about to involve nerve elements (C).
Reference
-
References
1. Albert TJ, Vacarro A. Postlaminectomy kyphosis. Spine (Phila Pa 1976). 23:2738–2745. 1998.2. Al-Mahfoudh R, Qattan E, Ellenbogen JR, Wilby M, Barrett C, Pigott T. Applications of the ultrasonic bone cutter in spinal surgery--our preliminary experience. Br J Neurosurg. 28:56–60. 2014.3. Bydon M, Macki M, Xu R, Ain MC, Ahn ES, Jallo GI. Spinal decompression in achondroplastic patients using high-speed drill versus ultrasonic bone curette: technical note and outcomes in 30 cases. J Pediatr Orthop. 34:780–786. 2014.4. Desai MJ, Padmanabhan G, Simbasivan A, Kamanga-Sollo GG, Dharmappa A. Directional preference following epidural steroid injection in three patients with acute cervical radiculopathy. Pain Pract. 13:559–565. 2013.5. Epstein NE. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg Neurol Int. 10:100. 2019.6. Fountas KN, Kapsalaki EZ, Nikolakakos LG, Smisson HF, Johnston KW, Grigorian AA, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976). 32:2310–2317. 2007.
Article7. Gokaslan ZL, Telfeian AE, Wang MY. Introduction: endoscopic spine surgery. Neurosurg Focus. 40:E1. 2016.
Article8. Halani SH, Baum GR, Riley JP, Pradilla G, Refai D, Rodts GE Jr, et al. Esophageal perforation after anterior cervical spine surgery: a systematic review of the literature. J Neurosurg Spine. 25:285–291. 2016.
Article9. Hazer DB, Yaşar B, Rosberg HE, Akbaş A. Technical aspects on the use of ultrasonic bone shaver in spine surgery: experience in 307 patients. Biomed Res Int. 2016:8428530. 2016.
Article10. Kim HS, Wu PH, Lee YJ, Kim DH, Kim JY, Lee JH, et al. Safe route for cervical approach: partial pediculotomy, partial vertebrotomy approach for posterior endoscopic cervical foraminotomy and discectomy. World Neurosurg. 140:e273–e282. 2020.
Article11. Klaassen Z, Tubbs RS, Apaydin N, Hage R, Jordan R, Loukas M. Vertebral spinal osteophytes. Anat Sci Int. 86:1–9. 2011.
Article12. Komp M, Oezdemir S, Hahn P, Ruetten S. Full-endoscopic posterior foraminotomy surgery for cervical disc herniations. Oper Orthop Traumatol. 30:13–24. 2018.
Article13. Lee DG, Park CK, Lee DC. Clinical and radiological results of posterior cervical foraminotomy at two or three levels: a 3-year follow-up. Acta Neurochir (Wien). 159:2369–2377. 2017.
Article14. Li ZZ, Cao Z, Zhao HL, Shang WL, Hou SX. Ultrasonic osteotome assisted full-endoscopic en block resection of thoracic ossified ligamentum flavum: technical note and 2 years follow-up. Pain Physician. 24:E239–E248. 2021.15. Massel DH, Mayo BC, Bohl DD, Narain AS, Hijji FY, Fineberg SJ, et al. Improvements in neck and arm pain following an anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 42:E825–E832. 2017.
Article16. Mok JK, Sheha ED, Samuel AM, McAnany SJ, Vaishnav AS, Albert TJ, et al. Evaluation of current trends in treatment of single-level cervical radiculopathy. Clin Spine Surg. 32:E241–E245. 2019.
Article17. Oh HS, Hwang BW, Park SJ, Hsieh CS, Lee SH. Percutaneous endoscopic cervical discectomy (PECD): an analysis of outcome, causes of reoperation. World Neurosurg. 102:583–592. 2017.
Article18. Papavero L, Kothe R. Minimally invasive posterior cervical foraminotomy for treatment of radiculopathy : an effective, time-tested, and cost-efficient motion-preservation technique. Oper Orthop Traumatol. 30:36–45. 2018.
Article19. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: a prospective, randomized, controlled study. Spine (Phila Pa 1976). 33:940–948. 2008.
Article20. Selvanathan SK, Beagrie C, Thomson S, Corns R, Deniz K, Derham C, et al. Anterior cervical discectomy and fusion versus posterior cervical foraminotomy in the treatment of brachialgia: the Leeds spinal unit experience (2008-2013). Acta Neurochir (Wien). 157:1595–1600. 2015.
Article21. Shriver MF, Lewis DJ, Kshettry VR, Rosenbaum BP, Benzel EC, Mroz TE. Dysphagia rates after anterior cervical diskectomy and fusion: a systematic review and meta-analysis. Global Spine J. 7:95–103. 2017.
Article22. Tong Y, Huang Z, Hu C, Fan Z, Bian F, Yang F, et al. A comparison study of posterior cervical percutaneous endoscopic ventral bony decompression and simple dorsal decompression treatment in cervical spondylotic radiculopathy caused by cervical foraminal and/or lateral spinal stenosis: a clinical retrospective study. BMC Musculoskelet Disord. 21:290. 2020.
Article23. Wan Q, Zhang D, Li S, Liu W, Wu X, Ji Z, et al. Posterior percutaneous full-endoscopic cervical discectomy under local anesthesia for cervical radiculopathy due to soft-disc herniation: a preliminary clinical study. J Neurosurg Spine. 29:351–357. 2018.
Article24. Xiao CM, Yu KX, Deng R, Long QY, Chu L, Xiong Y, et al. Modified Khole percutaneous endoscopic surgery for cervical foraminal stenosis: partial pediculectomy approach. Pain Physician. 22:E407–E416. 2019.25. Yamazaki S, Kokubun S, Ishii Y, Tanaka Y. Courses of cervical disc herniation causing myelopathy or radiculopathy: an analysis based on computed tomographic discograms. Spine (Phila Pa 1976). 28:1171–1175. 2003.
Article26. Ye ZY, Kong WJ, Xin ZJ, Fu Q, Ao J, Cao GR, et al. Clinical observation of posterior percutaneous full-endoscopic cervical foraminotomy as a treatment for osseous foraminal stenosis. World Neurosurg. 106:945–952. 2017.
Article27. Yu L, Wen JK, Wang S, Wang WH, Yu JM, Ye XJ. Removal of calcified lumbar disc herniation with endoscopic-matched ultrasonic osteotome - our preliminary experience. Br J Neurosurg. 34:80–85. 2020.
Article28. Yu Y, Jiang Y, Xu F, Mao Y, Yuan L, Li C. Percutaneous full-endoscopic C2 ganglionectomy for the treatment of intractable occipital neuralgia: technical note. Oper Neurosurg (Hagerstown). 21:E472–E478. 2021.
Article29. Zheng C, Huang X, Yu J, Ye X. Posterior percutaneous endoscopic cervical diskectomy: a single-center experience of 252 cases. World Neurosurg. 120:e63–e67. 2018.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Cervical Inclinatory Foraminotomy for Spondylotic Radiculopathy Preliminary
- Posterior Endoscopic Cervical Decompression: Review and Technical Note
- Endoscope Assisted Anterior Cervical Foraminotomy
- Posterior Cervical Microscopic Foraminotomy and Discectomy with Laser for Unilateral Radiculopathy
- Comparison of Surgical Results between Soft Ruptured Disc and Foraminal Stenosis Patients in Posterior Cervical Laminoforaminotomy
