Feasibility and reliability of various morphologic features on magnetic resonance imaging for iliotibial band friction syndrome
- Affiliations
-
- 1Department of Radiology, The Armed Forces Capital Hospital, Seongnam, Korea
- 2Department of Radiology, Severance Hospital, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2541029
- DOI: http://doi.org/10.3344/kjp.22399
Abstract
- Background
To evaluate the feasibility, inter-reader reliability, and intra-reader reliability for various morphological features reported to be related to iliotibial band friction syndrome (ITBFS) on knee magnetic resonance imaging (MRI).
Methods
A total of 145 patients with a clinical diagnosis and knee MRI findings consistent with ITBFS were included in the “study group” and 232 patients without knee pathology on both physical examination and MRI were included in the “control group”. Various morphologic features on knee MRI were assessed including the patella shape, patella height, lateral epicondyle anterior-posterior (AP) width, lateral epicondyle height, ITB diameter (ITB-d), and ITB area (ITB-a).
Results
Patients in the study group had significantly higher lateral epicondyle height (13.9 mm vs. 12.92 mm, P = 0.003), ITB-d (2.9 mm vs. 2.0 mm, P = 0.022), and ITB-a (38.5 mm2 vs. 23.8 mm2 , P < 0.001) than the control group. ITB-a showed higher area under the curve index (0.849 with 74.1% sensitivity and 72.4% specificity at a 30.3 mm2 cutoff) than ITB-d (0.710 with 70.8% sensitivity and 61.2% specificity at 2.4 mm cutoff) and lateral epicondyle height (0.776 with 72.4% sensitivity and 67.8% specificity at 13.4 mm cutoff). However, only the interreader agreement for ITB-a (intraclass correlation coefficient = 0.65) was moderate, while the agreements for other morphologic features were good or excellent.
Conclusions
Lateral epicondyle height seems to be a reliable and feasible morphologic feature for diagnosis of ITBFS.
Keyword
Figure
-
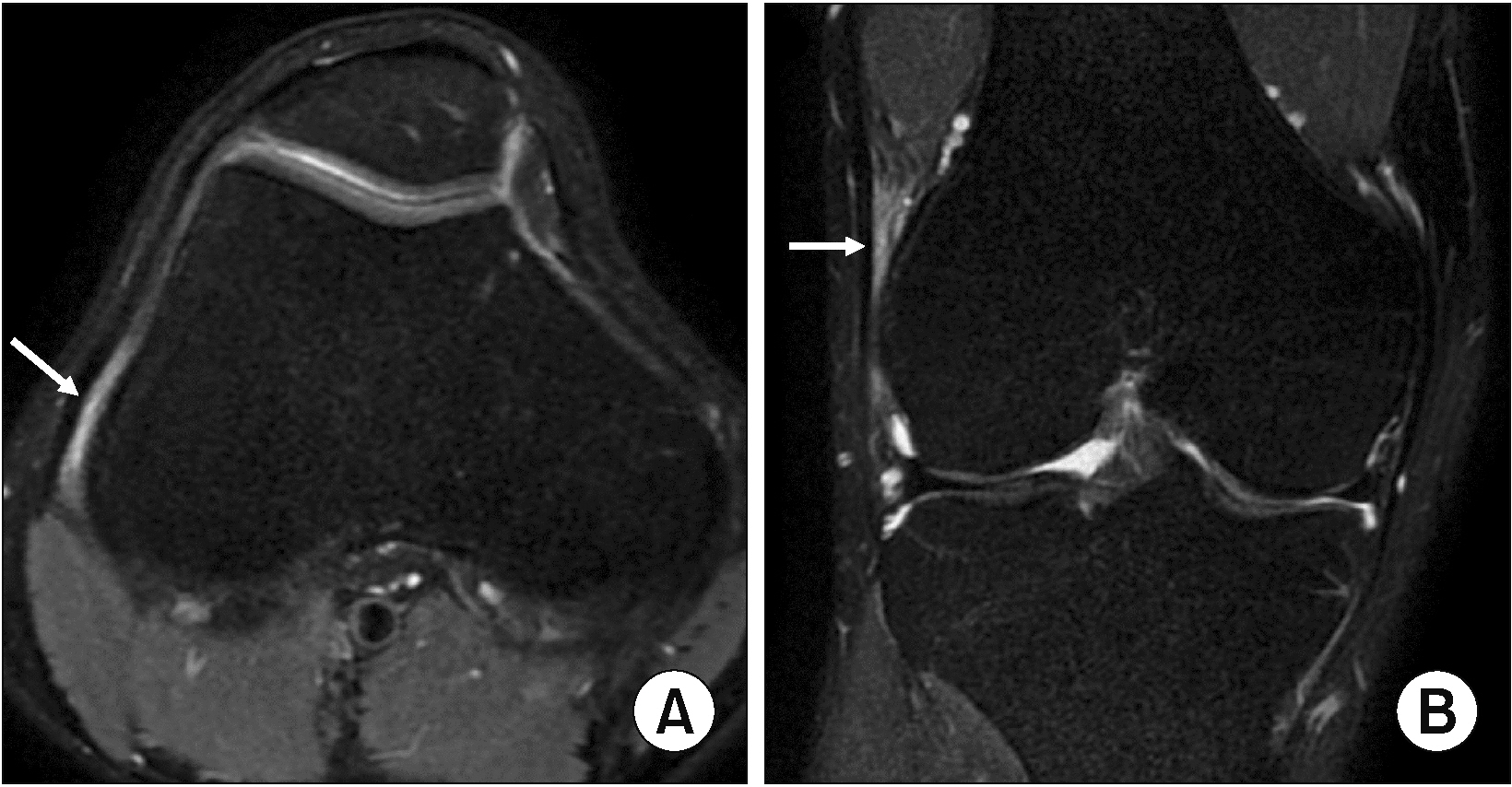
Fig. 1 Magnetic resonance imaging findings of iliotibial band friction syndrome (ITBFS). The white arrows demonstrate the increased signal intensity between the ITB and lateral femoral condyle on axial (A) and coronal (B) T2-weighted fat saturation images.

Fig. 2 Assessment of various morphologic findings on knee magnetic resonance imaging. Patella shape was determined on axial T2-weighted fat saturation (FS) images based on Wiberg classification: (A) type I = the medial and lateral facets of the patella are roughly symmetric and concave in shape, (B) type II = lateral facet is slightly longer than medial facet and usually concave shape of lateral facet, (C) type III = medial facet is markedly smaller with more vertical orientation.

Fig. 3 Assessment of various morphologic findings on knee magnetic resonance imaging. (A) Patella height was determined on sagittal T2-weighted fat saturation (FS) images according to Insall-Salvati ratio. (B) On axial T2-weighted FS images where the lateral epicondyle is the most prominent, lateral epicondyle antero-posterior (AP) width was measured by drawing the line connecting the lateral margin of the anterior and posterior articular surface of the lateral condyle. Then, the lateral epicondyle height was measured by drawing the line perpendicular to the first line toward the most lateral point on the lateral epicondyle (arrow).

Fig. 4 Assessment of various morphologic findings on knee magnetic resonance imaging. (A) Iliotibial band diameter (ITB-d) was measured in the thickest region at the level of lateral femoral epicondyle on axial T2-weighted fat saturation image. (B) On the same axial image plane, ITB area (ITB-a) was also measured by drawing free-hand region of interests at the thickest ITB.

Fig. 5 Receiver operating characteristic analysis to assess the performance of lateral epicondyle height, iliotibial band diameter (ITB-d), and ITB area (ITB-a) for predicting the risk of iliotibial band syndrome. (A) The area under curve (AUC)-index of ITB-d was 0.710 (95% confidence interval [CI]: 0.652–0.768). At a cutoff value of 2.4 mm, the sensitivity and specificity were 70.8% and 61.2%, respectively. (B) The AUC-index of lateral epicondyle height was 0.776 (95% CI: 0.723–0.829). At a cutoff value of 13.4 mm, the sensitivity and specificity were 72.4% and 67.8%, respectively. (C) The AUC-index of ITB-a was 0.849 (95% CI: 0.803–0.894). At a cutoff value of 30.3 mm2, the sensitivity and specificity were 74.1% and 72.4%, respectively.
Reference
-
1. Orava S. 1978; Iliotibial tract friction syndrome in athletes--an uncommon exertion syndrome on the lateral side of the knee. Br J Sports Med. 12:69–73. DOI: 10.1136/bjsm.12.2.69. PMID: 687887. PMCID: PMC1859635.2. Khaund R, Flynn SH. 2005; Iliotibial band syndrome: a common source of knee pain. Am Fam Physician. 71:1545–50. DOI: 10.53347/rid-49962. PMID: 15864895.3. Hong JH, Kim JS. 2013; Diagnosis of iliotibial band friction syndrome and ultrasound guided steroid injection. Korean J Pain. 26:387–91. DOI: 10.3344/kjp.2013.26.4.387. PMID: 24156006. PMCID: PMC3800712.4. Flato R, Passanante GJ, Skalski MR, Patel DB, White EA, Matcuk GR Jr. 2017; The iliotibial tract: imaging, anatomy, injuries, and other pathology. Skeletal Radiol. 46:605–22. DOI: 10.1007/s00256-017-2604-y. PMID: 28238018.5. Bankaoglu M, Mahmutoglu AS, Celebi I, Eren OT, Erturk SM, Kilic E, et al. 2018; Association of iliotibial band friction syndrome with patellar height and facets variations: a magnetic resonance imaging study. Iran J Radiol. 15:e63459. DOI: 10.5812/iranjradiol.63459.6. Everhart JS, Kirven JC, Higgins J, Hair A, Chaudhari AA, Flanigan DC. 2019; The relationship between lateral epicondyle morphology and iliotibial band friction syndrome: a matched case-control study. Knee. 26:1198–203. Erratum in: Knee 2020; 27: 1291. DOI: 10.1016/j.knee.2020.06.002. PMID: 32620349.7. Li J, Sheng B, Qiu L, Yu F, Lv FJ, Lv FR, et al. 2021; A quantitative MRI investigation of the association between iliotibial band syndrome and patellofemoral malalignment. Quant Imaging Med Surg. 11:3209–18. DOI: 10.21037/qims-20-1101. PMID: 34249647. PMCID: PMC8250009.8. Agridag Ucpinar B, Bankaoglu M, Eren OT, Erturk SM. 2021; Measurement of iliotibial band diameter in iliotibial band friction syndrome and comparison with an asymptomatic population. Acta Radiol. 62:1188–92. DOI: 10.1177/0284185120958407. PMID: 32938222.9. Park J, Cho HR, Kang KN, Choi KW, Choi YS, Jeong HW, et al. 2021; The role of the iliotibial band cross-sectional area as a morphological parameter of the iliotibial band friction syndrome: a retrospective pilot study. Korean J Pain. 34:229–33. DOI: 10.3344/kjp.2021.34.2.229. PMID: 33785675. PMCID: PMC8019960.10. Wibeeg G. 1941; Roentgenographs and anatomic studies on the femoropatellar joint: with special reference to chondromalacia patellae. Acta Orthop Scand. 12:319–410. DOI: 10.3109/17453674108988818.11. Insall J, Salvati E. 1971; Patella position in the normal knee joint. Radiology. 101:101–4. DOI: 10.1148/101.1.101. PMID: 5111961.12. Shabshin N, Schweitzer ME, Morrison WB, Parker L. 2004; MRI criteria for patella alta and baja. Skeletal Radiol. 33:445–50. DOI: 10.1007/s00256-004-0794-6. PMID: 15221214.13. McHugh ML. 2012; Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 22:276–82. DOI: 10.11613/BM.2012.031. PMID: 23092060. PMCID: PMC3900052.14. Bland JM, Altman DG. 1986; Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1:307–10. DOI: 10.1016/S0140-6736(86)90837-8. PMID: 2868172.15. Walbron P, Jacquot A, Geoffroy JM, Sirveaux F, Molé D. 2018; Iliotibial band friction syndrome: an original technique of digastric release of the iliotibial band from Gerdy's tubercle. Orthop Traumatol Surg Res. 104:1209–13. DOI: 10.1016/j.otsr.2018.08.013. PMID: 30341031.16. Foch E, Milner CE. 2019; Influence of previous iliotibial band syndrome on coordination patterns and coordination variability in female runners. J Appl Biomech. 35:305–11. DOI: 10.1123/jab.2018-0350. PMID: 31141437.17. Ekman EF, Pope T, Martin DF, Curl WW. 1994; Magnetic resonance imaging of iliotibial band syndrome. Am J Sports Med. 22:851–4. DOI: 10.1177/036354659402200619. PMID: 7856812.18. Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. 2000; Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 10:169–75. DOI: 10.1097/00042752-200007000-00004. PMID: 10959926.19. Messier SP, Edwards DG, Martin DF, Lowery RB, Cannon DW, James MK, et al. 1995; Etiology of iliotibial band friction syndrome in distance runners. Med Sci Sports Exerc. 27:951–60. DOI: 10.1249/00005768-199507000-00002. PMID: 7564981.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intra-Articular Fibroma of Tendon Sheath in a Knee Joint Associated with Iliotibial Band Friction Syndrome
- Diagnosis of Iliotibial Band Friction Syndrome and Ultrasound Guided Steroid Injection
- The role of the iliotibial band cross-sectional area as a morphological parameter of the iliotibial band friction syndrome: a retrospective pilot study
- External Snapping Hip Syndrome: Emphasis on the MR Imaging
- The role of the iliotibial band cross-sectional area as a morphological parameter of the iliotibial band friction syndrome: a retrospective pilot study
