Lung ultrasound for evaluation of dyspnea: a pictorial review
- Affiliations
-
- 1Department of Radiodiagnosis, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India
- 2Department of Pediatrics, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India
- 3Department of Pulmonary Medicine, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India
- KMID: 2540138
- DOI: http://doi.org/10.4266/acc.2022.00780
Abstract
- Lung ultrasound is based on the analysis of ultrasound artifacts generated by the pleura and air within the lungs. In recent years, lung ultrasound has emerged as an important alternative for quick evaluation of the patient at the bedside. Several techniques and protocols for performing lung ultrasound have been described in the literature, with the most popular one being the Bedside Lung Ultrasound in Emergency (BLUE) protocol which can be utilized to diagnose the cause of acute dyspnea at the bedside. We attempt to provide a simplified approach to understanding the physics behind the artifacts used in lung ultrasound, the imaging techniques, and the application of the BLUE protocol to diagnose the commonly presenting causes of acute dyspnea.
Keyword
Figure
-

Figure 1. (A) Reverberation artifacts [2]. When two reflective parallel interfaces lie in the path of the ultrasound beam, the beam gets reflected multiple times between these interfaces. Hence, the transducer assumes them to arise at increasing depths depending on the time delay between transmitted pulse and received echo. This generates an image comprising of multiple echogenic parallel lines placed equidistant from each other, which decrease in brightness with increasing depth. In the chest, the pleural line lies parallel to the probe and acts as a reflective interface when the lungs are aerated, giving rise to reverberation artifacts known as “A-lines” due to repetitive reflections between it and the transducer. Hence, the presence of A-lines denotes an aerated lung. It is important to note that tissue harmonic imaging (THI) will decrease this artifact. (B) Comet-tail artifacts [3]. These are a subtype of reverberation artifacts arising from highly reflective, closely apposed interfaces like calcium, cholesterol crystals, and metal, which cannot be resolved separately. The comet-tail artifact appears as a tapering echogenic cone, showing decreased amplitude and width with increasing depths. Previously, the B-lines were called comet-tail artifacts. (C) Ring-down artifacts [2]. These are similar to comet-tail artifacts but arise from fluid trapped between air. B-lines have been described to be ring-down artifacts. Comet-tail and ring-down artifacts are minimized by spatial compound imaging, which needs to be turned off to get less divergent, sharper, and brighter B-lines. THI also assists in producing sharper comet tails. Permission obtained from RSNA to reproduce images in print or web.

Figure 2. Focused transthoracic ultrasound using 14-zone scanning protocol by Laursen et al. [6], based on principles of Lichtenstein and Volpicelli, using a curved array low-frequency transducer placed in a longitudinal axis over an intercostal space with the patient in a supine position. (A) Zone R1: transducer placed in the 2nd intercostal space, a few centimeters away from the sternum. (B) Zone R2: transducer placed in the 4th intercostal space in the mid-clavicular line. (C) Zone R3: transducer placed in the mid-axillary line on the lower part of the lateral chest, in approximately the 5th or 6th intercostal space. (D) Zone R4: transducer placed in the mid-axillary line on the upper part of the lateral chest, in the 3rd intercostal space. (E) Zone R5: with the patient in a sitting position, the posterior chest wall is scanned by placing the transducer on the lower part of the chest along a vertical line passing through the inferior angle of the scapula. (F) Zone R6: the transducer is placed medially in the posterior midclavicular line at a level corresponding to middle to lower part of the scapula. (G) Zone R7: transducer placed further cranially, medial to the upper part of the scapula. Similarly, scanning is done on the left side in zones L5–L7. (H) Zone 8 scanning of anterolateral chest wall proposed by Volpicelli et al. Zones are divided into anterior and lateral by the parasternal line (PSL), anterior axillary line (AAL), posterior axillary line (PAL), and upper and basal by a line passing below/at the level of the nipple-areola complex. Zone 1: anterior upper; zone 2: anterior basal; zone 3: lateral upper; zone 4: lateral basal.

Figure 3. Localizing the bedside lung ultrasound in emeregency (BLUE) points [7]. (A) The radiologist first compares their hands with the patient's and places one hand just below the clavicle with fingertips at the midline. The “upper BLUE point” is located at the root of the middle and ring fingers. The other hand is applied just below the upper one, excluding the thumb. The “lower BLUE point” is located in the middle of the palm of the lower hand with the inferior edge of the little finger indicating the “phrenic line.” (B) The “posterolateral alveolar and/or pleural syndrome (PLAPS) point” which lies at the intersection of the posterior continuation of lower BLUE point and posterior axillary line, is used to scan the posterior lung zones in a critically ill patient in supine/semi-recumbent position. It is best performed with a small footprint probe (C, D) which is held like a tennis racket, placed perpendicular to the PLAPS point, and directed as cranially as possible for a wider scanning window.

Figure 4. (A) Longitudinal ultrasound scan of the second intercostal space in the mid-clavicular line on anterior chest wall depicting sonographic appearance of normal lung, identified by the landmarks forming the “bat sign”: two ribs (R) with posterior acoustic shadowing representing the wings of the bat, and the hyperechoic pleural line (asterisk), its body. A-lines (arrowheads) can be seen parallel to the pleural line. (B) Cine US clip depicting the same (Supplementary Material 1).

Figure 5. Lung sliding. (A) M-mode with the cursor over the pleural line illustrating the “seashore sign.” The motionless portion of the chest above the pleural line creates horizontal “waves,” (bracket) and the lung sliding below the pleural line creates a granular pattern, the “sand” (brace). (B) Cine US clip demonstrating the same (Supplementary Material 2).

Figure 6. The presence of lung sliding and A-lines constitutes the A-profile [7]. This is followed by sequential venous analysis to look for thrombosed veins (pulmonary embolism) or assessment of posterolateral alveolar and/or pleural syndrome (PLAPS) point in case of free veins to diagnose pneumonia (PLAPS) and chronic obstructive pulmonary disease (COPD)/asthma (no PLAPS). BLUE: bedside lung ultrasound in Emergency.

Figure 7. A profile. Sagittal greyscale ultrasound scans (A-H) of eight lung zones in bilateral anterolateral chest wall revealing the A-profile A-lines with lung sliding and absence of B-lines in a 30-year-old afebrile male with a history of chronic cigarette smoking, presenting with dyspnea, diagnosed as exacerbation of chronic obstructive pulmonary disease/asthma on ultrasound. (I) Findings on chest X-ray were seen to be concordant. Bilateral lung fields appear hyperinflated with rounded costophrenic angles and flattening of hemidiaphragm.

Figure 8. (A) Longitudinal scan of anterior chest wall showing 3 “B-lines”: comet-tail artifacts, always arising from the pleural line, and always moving in synchrony with lung-sliding. They are almost always long, well-defined, laser-like, hyperechoic, erasing A-lines, and are considered significant when ≥3. Few B-lines may be normally seen in basal lung zones. (B) Cine US clip demonstrating the same (Supplementary Material 3).
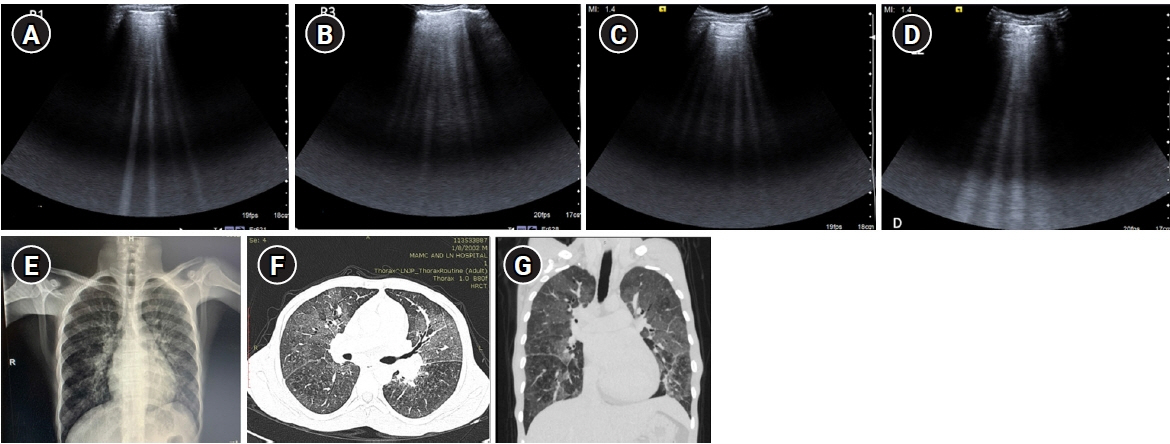
Figure 9. B-profile. Diffuse interstitial syndrome on ultrasound, diagnosed by the presence of multiple (≥3) B-lines in >1 scanning zone in anterolateral chest wall on each side in a patient presenting with acute dyspnea and hemoptysis. (A, B) Four B-lines are known as “septal rocket” pattern and represent interlobular septal thickening. (C, D) Five or more B-lines are called “ground glass rocket” patterns, representing ground-glass areas on the computed tomography of the chest. the pleural line in this case was regular in appearance. The patient was diagnosed with pulmonary edema based on ultrasound findings. (E) Chest X-ray revealed concordant findings in the form of cephalization of the pulmonary vasculature and prominent interstitial markings. Axial (F) and coronal (G) sections from contrast-enhanced chest computed tomography scan performed in the patient revealed ground glass opacities and Interlobular septal thickening as demonstrated by the “ground glass rocket” pattern and “septal rocket” pattern respectively on ultrasound, providing further confirmation of the diagnosis.

Figure 10. An abolished lung sliding combined with “A-line sign” (exclusive A-lines with absence of B-lines) is assigned the A’ profile [7]. Detection of “lung point” confirms the diagnosis as pneumothorax. If Lung point is not demonstrated, the patient would require further diagnostic modalities for assessment. BLUE: bedside lung ultrasound in Emergency.
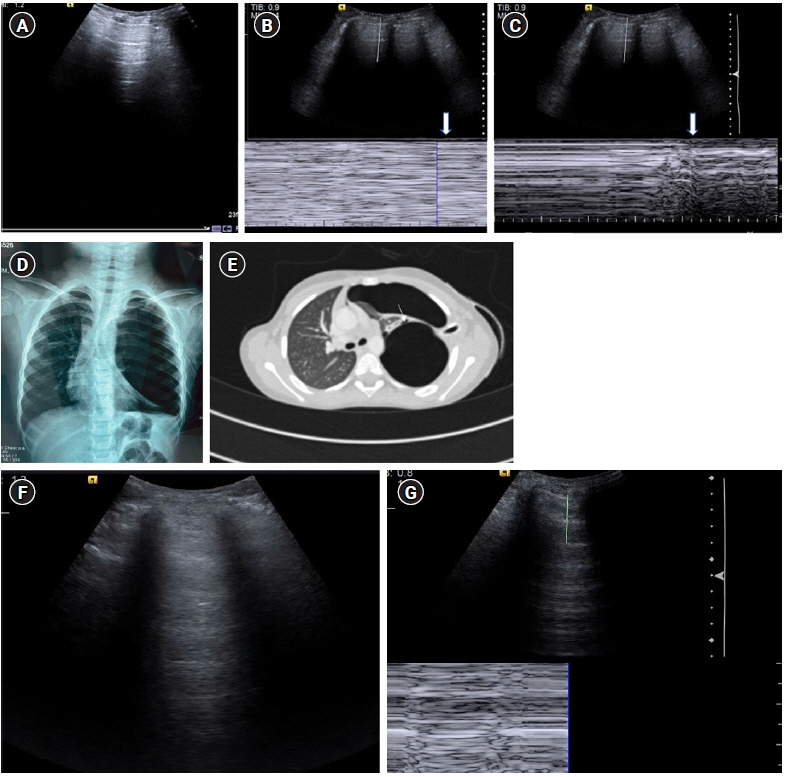
Figure 11. (A-E) A’ profile. Sagittal grey scale ultrasound scan (A) with M-mode tracing (B) in a 6-year old boy with history of dyspnea, chest pain and previous intercostal chest tube drainage for empyema revealed abolished lung sliding in the form of “stratosphere sign”: horizontal lines above and below the pleural line, in the left anterior and lateral lung zones with presence of A-lines and absent B-lines (known as A’ profile). (C) Diagnosis of pneumothorax was confirmed on ultrasound by localizing the “lung point”: visualizing intermittent stratosphere sign and seashore sign (arrows). The lung point was however visualized in posterolateral lung zones, indicating a large pneumothorax. (D) Chest X-ray in the same patient revealed a large left sided pneumothorax with contralateral tracheomediastinal shift, further confirming the findings of a large pneumothorax as diagnosed on ultrasound. The patient was however hemodynamically stable. (E) Contrast-enhanced chest computed tomography scan chest revealed a bronchopleural fistula (arrow). (F) Cine US clip showing absent lung sliding (Supplementary Material 4). (G) Cine US clip showing “stratosphere sign (Supplementary Material 5).”
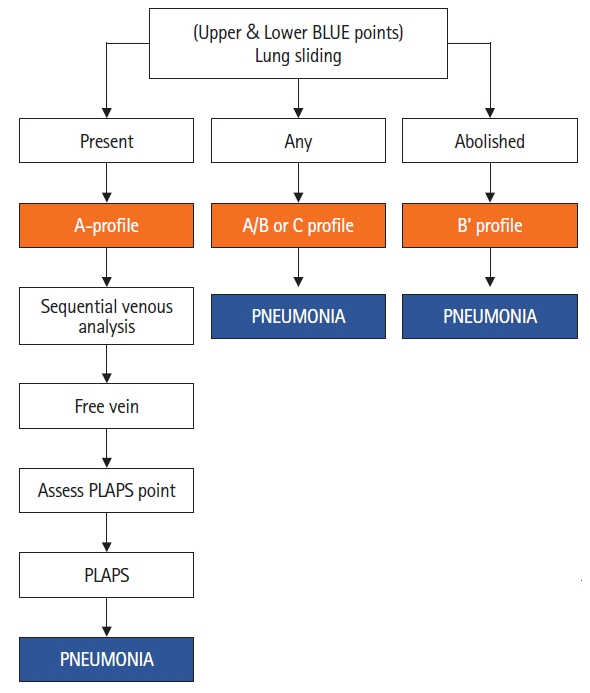
Figure 12. Anterior consolidation is called the C profile [7]. Unilateral B-lines (atleast 3 in one scanning zone) with A lines on the contralateral side is called the A/B profile. An abolished lung sliding combined with B lines is called B’ profile. Meanwhile, A-profile anteriorly with presence of posterolateral consolidation is called the A-no V-PLAPS profile. BLUE: bedside lung ultrasound in Emergency; PLAPS: posterolateral alveolar and/or pleural syndrome.

Figure 13. C profile. (A) Greyscale sagittal ultrasound scan of the right upper anterolateral chest in a 13-year-old female presenting with dyspnea, fever, and cough demonstrating “translobar consolidation” identified by “tissue-like” echotexture, absence of A-lines, presence of sonographic air-bronchograms and a lack of a shredded border. (B) Colour doppler revealed the presence of internal vascularity. (C) Right upper lobe consolidation with air bronchograms was similarly noted on Chest X-ray, correlating with the ultrasound findings.

Figure 14. posterolateral alveolar and/or pleural syndrome profile. (A) Pleural effusion (asterisk) in a 20-year-old female presenting with breathlessness and chest pain identified by visualizing the underlying visceral pleural line/“lung line” (arrow). “Quad sign,” a sonographic feature is depicted in the form of a rough quadrilateral bounded by the two ribs (R) with their posterior acoustic shadow on either side, the pleural line superiorly, and the lung line inferiorly. (B) M-mode tracing in a pleural effusion reveals a “sinusoidal” pattern. The underlying lung appears to be normal, with few Sub-B lines seen.

Figure 15. (A) Greyscale sagittal ultrasound scan of the right upper lateral chest in a 25-year-old male presenting with dyspnea, fever, and cough demonstrating “non-translobar consolidation”/“fractal sign” identified by “tissue-like” echotexture, absence of A-lines with an underlying shredded border. (B) Three B-lines representing the “lung rocket” pattern were noted only on the left side. Unilateral lung rockets are seen in pneumonia. (C) Chest X-ray revealed fluffy air space opacities in bilateral lung fields (left>right). The patient was diagnosed with pneumonia.
Reference
-
1. Lichtenstein DA. BLUE protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill. Chest. 2015; 147:1659–70.2. Feldman MK, Katyal S, Blackwood MS. US artifacts. Radiographics. 2009; 29:1179–89.
Article3. Baad M, Lu ZF, Reiser I, Paushter D. Clinical significance of US artifacts. Radiographics. 2017; 37:1408–23.
Article4. Gargani L, Volpicelli G. How I do it: lung ultrasound. Cardiovasc Ultrasound. 2014; 12:25.
Article5. Jambrik Z, Monti S, Coppola V, Agricola E, Mottola G, Miniati M, et al. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. Am J Cardiol. 2004; 93:1265–70.
Article6. Laursen CB, Rahman NM, Volpicelli G. Thoracic ultrasound. Lausanne: European Respiratory Society;2018.7. Lichtenstein D. Lung ultrasound in the critically ill: The BLUE protocol. Switzerland: Springer;2016.8. Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling out pneumothorax in the critically ill: lung sliding. Chest. 1995; 108:1345–8.
Article9. Zanobetti M, Scorpiniti M, Gigli C, Nazerian P, Vanni S, Innocenti F, et al. Point-of-care ultrasonography for evaluation of acute dyspnea in the ED. Chest. 2017; 151:1295–301.
Article10. Volpicelli G, Mussa A, Garofalo G, Cardinale L, Casoli G, Perotto F, et al. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am J Emerg Med. 2006; 24:689–96.
Article11. Reissig A, Kroegel C. Transthoracic sonography of diffuse parenchymal lung disease: the role of comet tail artifacts. J Ultrasound Med. 2003; 22:173–80.12. Gargani L, Doveri M, D'Errico L, Frassi F, Bazzichi ML, Delle Sedie A, et al. Ultrasound lung comets in systemic sclerosis: a chest sonography hallmark of pulmonary interstitial fibrosis. Rheumatology (Oxford). 2009; 48:1382–7.
Article13. Copetti R, Copetti P, Soldati G. Ultrasound pattern in pulmonary fibrosis: have the vertical artifacts disappeared? Ultrasound Med Biol. 2010; 36:356–7.
Article14. Reissig A, Copetti R. Lung ultrasound in community-acquired pneumonia and in interstitial lung diseases. Respiration. 2014; 87:179–89.
Article15. Buda N, Piskunowicz M, Porzezińska M, Kosiak W, Zdrojewski Z. Lung ultrasonography in the evaluation of interstitial lung disease in systemic connective tissue diseases: criteria and severity of pulmonary fibrosis: analysis of 52 patients. Ultraschall Med. 2016; 37:379–85.16. Gargani L. Lung ultrasound: a new tool for the cardiologist. Cardiovasc Ultrasound. 2011; 9:6.
Article17. Lichtenstein D. Whole body ultrasonography in the critically ill. Heidelberg, Berlin, New York: Springer-Verlag;2010.18. Brusasco C, Santori G, Bruzzo E, Trò R, Robba C, Tavazzi G, et al. Quantitative lung ultrasonography: a putative new algorithm for automatic detection and quantification of B-lines. Crit Care. 2019; 23:288.
Article19. Lichtenstein D, Mezière G, Biderman P, Gepner A. The "lung point": an ultrasound sign specific to pneumothorax. Intensive Care Med. 2000; 26:1434–40.
Article20. De Luca C, Valentino M, Rimondi MR, Branchini M, Baleni MC, Barozzi L. Use of chest sonography in acute-care radiology. J Ultrasound. 2008; 11:125–34.
Article21. Murphy M, Nagdev A, Sisson C. Lack of lung sliding on ultrasound does not always indicate a pneumothorax. Resuscitation. 2008; 77:270.
Article22. Ball CG, Kirkpatrick AW, Feliciano DV. The occult pneumothorax: what have we learned? Can J Surg. 2009; 52:E173–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prenatal Diagnosis and Outcome of Congenital Lung Mass
- Fracture Detection with Ultrasonography in Multiple Bony Structures
- Role of ultrasound in the evaluation of first-trimester pregnancies in the acute setting
- Lung Ultrasound (in the Critically Ill) Superior to CT: the Example of Lung Sliding
- Pediatric lung ultrasound: its role in the perioperative period
