Lung Ultrasound (in the Critically Ill) Superior to CT: the Example of Lung Sliding
- Affiliations
-
- 1Hôpital Ambroise-Paré (Medical ICU), Paris-Ouest university, Boulogne, France. D.Licht@free.fr
- KMID: 2371148
- DOI: http://doi.org/10.4266/kjccm.2016.00955
Abstract
- This review article shows the potential of lung ultrasound in the critically ill (LUCI) to study lung sliding and describes the optimal equipment for its assessment. Then, it analyses the integration of lung sliding within lung ultrasound then whole body critical ultrasound. It describes the place of lung sliding in the BLUE-protocol (bedside lung ultrasound in emergency) (lung and venous ultrasound for diagnosing acute respiratory failure), the FALLS-protocol (fluid administration limited by lung sonography) (the role of lung sliding in circulatory failure), and the SESAME-protocol (sequential assessment of sonography assessing mechanism or origin of severe shock of indistinct cause) (whole body ultrasound in cardiac arrest). In the LUCIFLR project (LUCI favoring limitation of radiations), the consideration of lung sliding allows drastic reduction in irradiation and costs. In conclusion, lung sliding is proposed as a gold standard for indicating the presence of the lung at the chest wall and its correct expansion.
Keyword
Figure
-
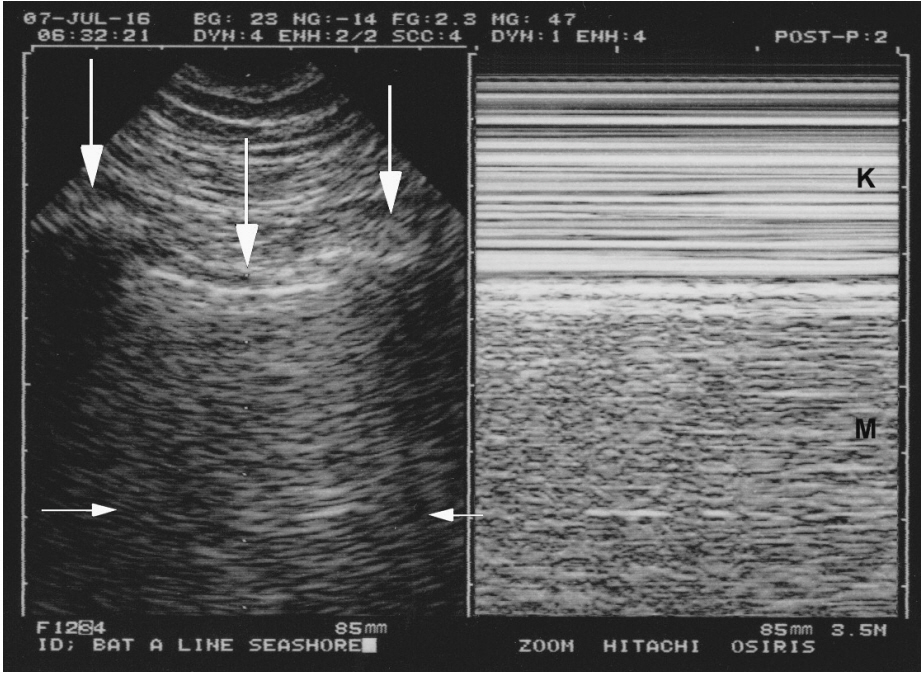
Figure 1. Normal lung sliding. Left, real time. Both ribs (lateral vertical arrows) and the pleural line (middle vertical arrow) outline the bat sign. In this adult, the pleural line is 0.5 cm below the rib line, allowing a confident recognition. Note one A-line partially visible (horizontal arrows) at the expected location (distance skin/pleural line). Right, M-mode. Lung sliding, not visible in the left (frozen) image, appears as a sandy pattern at and below the pleural line. This image shows two rectangular areas: from top to bottom, Keye’s space (soft tissues) (K) and Merlin’s space (the “lung”) (M). These areas are strictly separated by the pleural line. Note that this smart technology (1992) displays the pleural line of the left and right images at the same level.

Figure 2. B-lines and lung rockets. Typical multiple B-lines. This figure shows the 7 features of the B-line. Three are constant. 1) A comet-tail artifact. 2) It always arises from the pleural line. 3) It always moves in concert with lung sliding (and is therefore motionless if lung sliding is abolished). A video of B-profile and B’- profile is available at www.CEURF.net for this dynamic pattern. Four features are nearly always present: 4) long; 5) well-defined; 6) erasing A-lines; 7) and hyperechoicity. This definition allows recognition in any circumstances and avoids any confusion with other comet-tail artifacts. More than two B-lines between two ribs are called lung rockets, which are used to diagnose interstitial syndrome. Three or four B-lines are called septal rockets and correlate with edematous subpleural interlobular septa. The double, like here (at least seven) are called ground-glass rockets and correlate with computerized tomography ground glass areas. Diffuse lung rockets define the B-profile or the B’-profile (depending on the presence or absence of lung sliding).
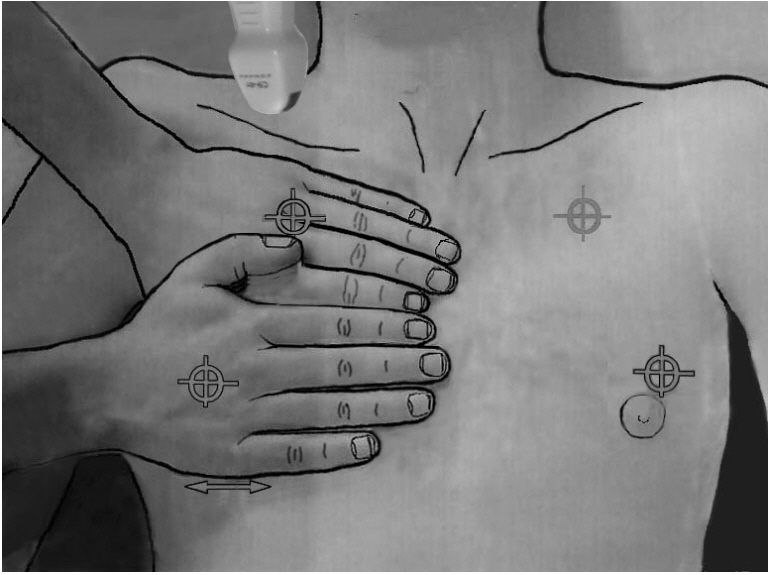
Figure 3. The BLUE-points. This image shows how the two hands (from the patient’s size) are placed in order to produce a projection of the lung (the lower arrow indicates the usual location of the diaphragm). The upper point (upper BLUE-point) would show a discrete lung sliding. The lower point (lower BLUE-point) is the usual site for assessing the amplitude of lung sliding (maximal at the base). Lung sliding will be minimal at the upper BLUE-point and usually null at the apex (see how a microconvex probe can be inserted at the right apex). The PLAPS-point is the transversal continuation of the lower BLUE-point, performed posteriorly to the posterior axillary line. BLUE: bedside lung ultrasound in emergency; PLAPS: posterolateral alveolar and/or pleural syndrome.
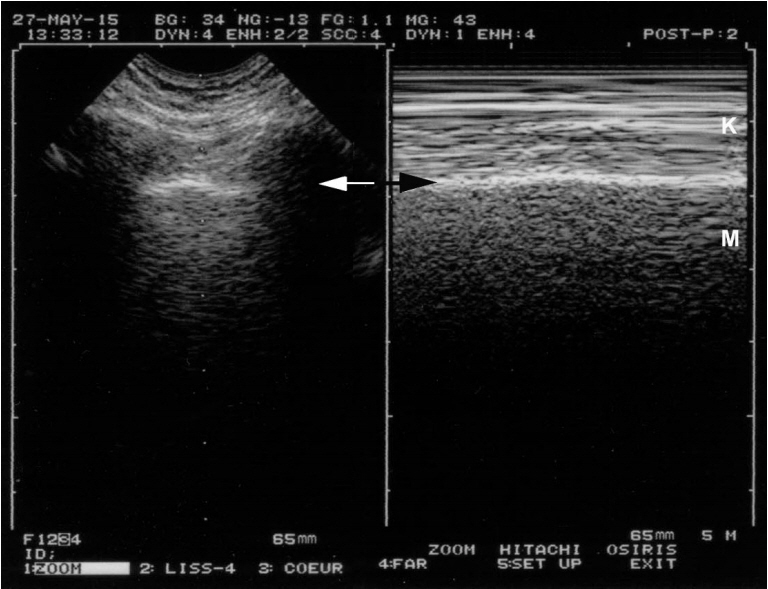
Figure 4. Lung sliding and dyspnea. On a frozen image, one can see that this patient is dyspneic. The left image allows localization of the pleural line (arrow). This location is reported at the right, allowing precise identification of the pleural line on Mmode (arrow). Keye’s space is not as homogeneous as in Figure 1, as artifacts are caused by the recruitment of accessory respiratory muscles. Note however that the patterns of the two areas (Keye’s and Merlin’s spaces) are different, and lung sliding is easily identifiable.
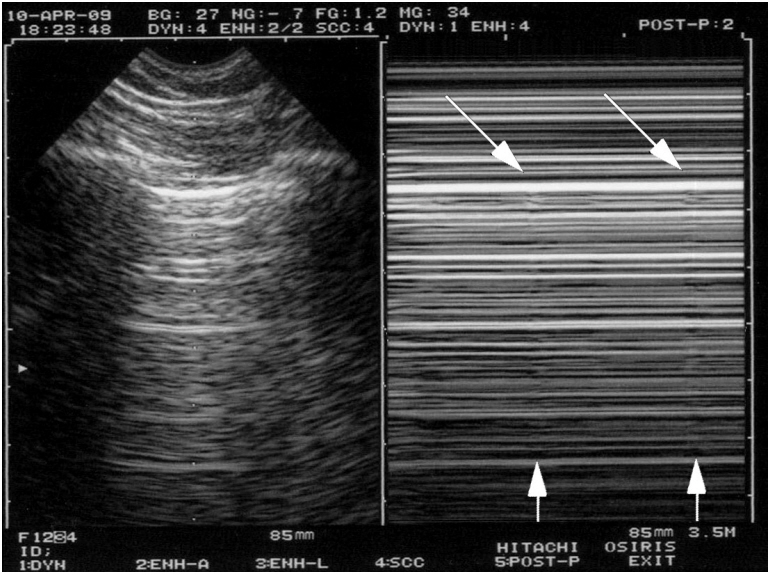
Figure 5. Extremely weak lung sliding in ventilated patients. The concept of the T-lines shows how subtle lung ultrasound can be. In the first view, this double image indicates pneumothorax: A-lines with a stratosphere sign. In reality, this is not a pneumothorax. This image is of a sedated patient with protective ventilation (low tidal volume); at the upper BLUE-point, all conditions for making lung sliding very discrete. The indications that the finding is not truly a pneumothorax are first because the image is not sufficient: if there is no lung point, it is too early to speak of pneumothorax. Second and most importantly, the oblique arrows show extremely subtle artifacts arising from the pleural line, and the vertical arrows show something like a vertical line (oblique arrows for not spoiling the subtle pattern). These are the T-lines and are an equivalent of the lung pulse. This extreme case shows that lung ultrasound can be compared with the subtle semiotics of ECG when a ventricular tachycardia is sought. BLUE: bedside lung ultrasound in emergency; ECG: electrocardiogram.
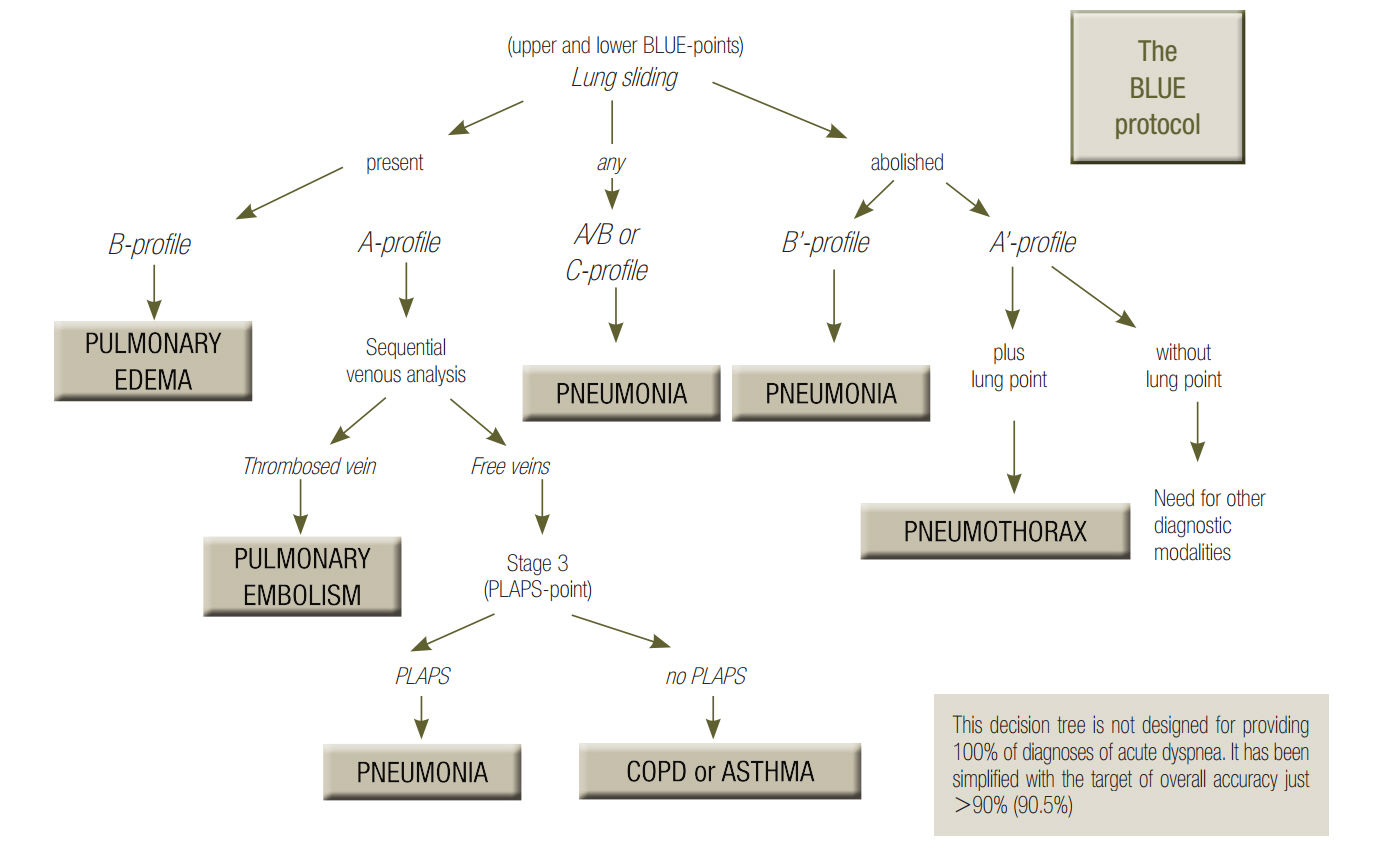
Figure 6. BLUE-protocol decision tree. This decision tree may appear complex, but the investment is worth it, since it provides the main diagnoses of acute respiratory failure with high accuracy. For going more in details, a whole book was necessary [3], but this decision tree makes a nice initial basis. One can see the lung sliding, at the very top. On an initial scan, abolished lung sliding might immediately suggest pneumothorax if it is associated with A-lines (the A’-profile) or pneumonia or ARDS if it is associated with lung rockets (the B’- profile). Adopted from reference [6]. ARDS: acute respiratory distress syndrome; BLUE: bedside lung ultrasound in emergency; PLAPS: posterolateral alveolar and/or pleural syndrome.
Reference
-
References
1. Friedman J. Diagnostic procedures in respiratory diseases. Harrison’s principles of internal medicine. 12th ed. New York: McGraw-Hill;1992. p. 1043.2. Lichtenstein DA. Lung ultrasound in the critically ill. Ann Intensive Care. 2014; 1.
Article3. Lichtenstein DA. Lung Sliding. Lung Ultrasound in the Critically Ill - the BLUE-protocol. 6th ed. Heidelberg: Springer-Verlag International;2016. p. 67–78.4. Lichtenstein DA, Mezière GA. The BLUE-points: three standardized points used in the BLUE-protocol for ultrasound assessment of the lung in acute respiratory failure. Crit Ultrasound J. 2011; 3:109–10.
Article5. Guyton AC, Hall JE. Textbook of medical physiology. 9th ed. Philadelphia: W.B. Saunders Company;1996. p. 496–7.6. Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE-protocol. Chest. 2008; 134:117–25.7. van der Werf TS, Zijlstra JG. Ultrasound of the lung: just imagine. Intensive Care Med. 2004; 30:183–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lung Ultrasound in Critically Ill Patients
- Usefulness of transthoracic lung ultrasound for the diagnosis of mild pneumothorax
- Lung Ultrasound in the Critically Ill
- Pediatric lung ultrasound: its role in the perioperative period
- Lung Cancer in patients with Idiopathic Pulmonary Fibrosis: Frequency and CT Findings
