Pediatric lung ultrasound: its role in the perioperative period
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. goingridgo@gmail.com
- KMID: 2436050
- DOI: http://doi.org/10.17085/apm.2018.13.1.18
Abstract
- There have been a number of recent advancements in the field of point-of-care ultrasound, including lung ultrasound for adult and pediatric populations. Evidence-based guidelines on the use of point-of-care lung ultrasound have been published. Lung ultrasound is superior to chest radiography in diagnosing several disorders of vital importance in the perioperative period. This review presents a discussion of techniques and clinical applications of lung ultrasound in pediatric patients focusing on usage in the perioperative period.
Keyword
MeSH Terms
Figure
-

Fig. 1 Lung ultrasound scan in a 2-year-old boy using a high-frequency (5–10 MHz) linear transducer. Each hemithorax is divided into six regions using three longitudinal lines (parasternal, anterior, and posterior axillary) and two axial lines (one above the diaphragm and the other 1 cm above the nipples). Twelve regions of the lungs are scanned sequentially from right to left, cranial to caudal, and anterior to posterior. The figure shows scanning of the right hemithorax.

Fig. 2 Image of A-lines and B-lines on lung ultrasound. A-lines are horizontal lines parallel to the pleural line, whereas B-lines are vertical lines originating from the pleural line and reaching the bottom of the screen.
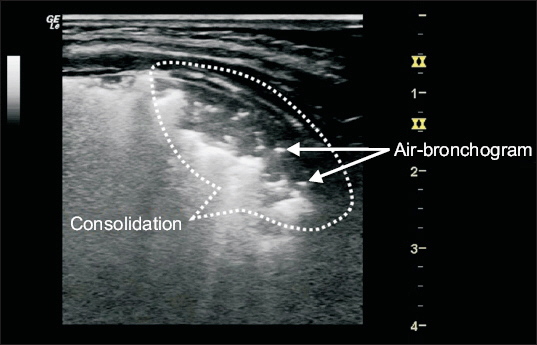
Fig. 3 Image of lung consolidations on lung ultrasound. Air bronchograms are observed within the consolidation.
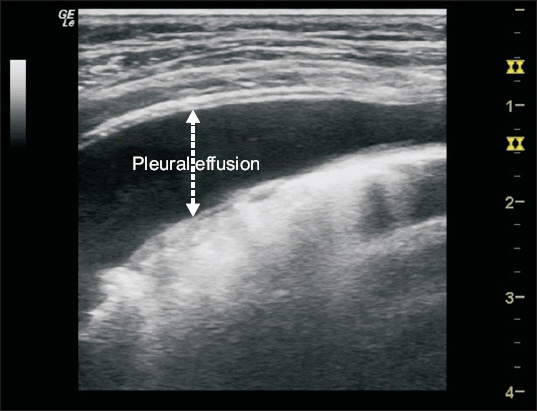
Fig. 4 Image of pleural effusion on lung ultrasound. A simple pleural effusion appears as a homogenous hypoechoic space between the parietal and visceral pleurae.
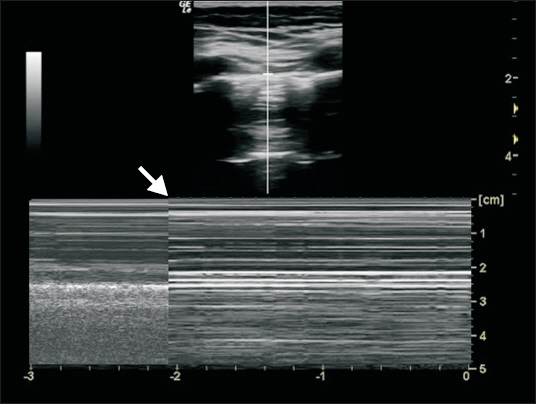
Fig. 5 Lung point on motion mode (M-mode). The arrow indicates a transition between a seashore sign (normal lung) and barcode sign (pneumothorax).
Reference
-
1. Lichtenstein D, Mezière G. A lung ultrasound sign allowing bedside distinction between pulmonary edema and COPD: the comet-tail artifact. Intensive Care Med. 1998; 24:1331–4. DOI: 10.1007/s001340050771. PMID: 9885889.2. Lichtenstein D, Mezière G, Biderman P, Gepner A. The “lung point”: an ultrasound sign specific to pneumothorax. Intensive Care Med. 2000; 26:1434–40. DOI: 10.1007/s001340000627. PMID: 11126253.3. Lichtenstein DA, Lascols N, Prin S, Mezière G. The “lung pulse”: an early ultrasound sign of complete atelectasis. Intensive Care Med. 2003; 29:2187–92. DOI: 10.1007/s00134-003-1930-9. PMID: 14557855.4. Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling out pneumothorax in the critically ill. Lung sliding. Chest. 1995; 108:1345–8. DOI: 10.1378/chest.108.5.1345. PMID: 7587439.5. Copetti R, Cattarossi L. The ‘double lung point’: an ultrasound sign diagnostic of transient tachypnea of the newborn. Neonatology. 2007; 91:203–9. DOI: 10.1159/000097454. PMID: 17377407.6. Caiulo VA, Gargani L, Caiulo S, Moramarco F, Latini G, Gargasole C, et al. Usefulness of lung ultrasound in a newborn with pulmonary atelectasis. Pediatr Med Chir. 2011; 33:253–5. PMID: 22428435.7. Caiulo VA, Gargani L, Caiulo S, Fisicaro A, Moramarco F, Latini G, et al. Lung ultrasound in bronchiolitis: comparison with chest X-ray. Eur J Pediatr. 2011; 170:1427–33. DOI: 10.1007/s00431-011-1461-2. PMID: 21468639.8. Copetti R, Cattarossi L. Ultrasound diagnosis of pneumonia in children. Radiol Med. 2008; 113:190–8. DOI: 10.1007/s11547-008-0247-8. PMID: 18386121.9. Copetti R, Cattarossi L, Macagno F, Violino M, Furlan R. Lung ultrasound in respiratory distress syndrome: a useful tool for early diagnosis. Neonatology. 2008; 94:52–9. DOI: 10.1159/000113059. PMID: 18196931.10. Darge K, Chen A. Point-of-care ultrasound in diagnosing pneumonia in children. J Pediatr. 2013; 163:302–3. DOI: 10.1016/j.jpeds.2013.04.059. PMID: 23796342.11. Piastra M, Yousef N, Brat R, Manzoni P, Mokhtari M, De Luca D. Lung ultrasound findings in meconium aspiration syndrome. Early Hum Dev. 2014; 90(Suppl 2):S41–3. DOI: 10.1016/S0378-3782(14)50011-4.12. Vergine M, Copetti R, Brusa G, Cattarossi L. Lung ultrasound accuracy in respiratory distress syndrome and transient tachypnea of the newborn. Neonatology. 2014; 106:87–93. DOI: 10.1159/000358227. PMID: 24819542.13. Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD, et al. Guidelines for performing ultrasound guided vascular cannulation: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2011; 24:1291–318. DOI: 10.1016/j.echo.2011.09.021. PMID: 22115322.14. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012; 38:577–91. DOI: 10.1007/s00134-012-2513-4. PMID: 22392031.15. Cattarossi L. Lung ultrasound: its role in neonatology and pediatrics. Early Hum Dev. 2013; 89(Suppl 1):S17–9. DOI: 10.1016/S0378-3782(13)70006-9.16. Acosta CM, Maidana GA, Jacovitti D, Belaunzarán A, Cereceda S, Rae E, et al. Accuracy of transthoracic lung ultrasound for diagnosing anesthesia-induced atelectasis in children. Anesthesiology. 2014; 120:1370–9. DOI: 10.1097/ALN.0000000000000231. PMID: 24662376.17. Cantinotti M, Giordano R, Valverde I. Lung ultrasound: a new basic, easy, multifunction imaging diagnostic tool in children undergoing pediatric cardiac surgery. J Thorac Dis. 2017; 9:1396–9. DOI: 10.21037/jtd.2017.05.71. PMID: 28740641. PMCID: PMC5506126.18. Bouhemad B, Mongodi S, Via G, Rouquette I. Ultrasound for “lung monitoring” of ventilated patients. Anesthesiology. 2015; 122:437–47. DOI: 10.1097/ALN.0000000000000558. PMID: 25501898.19. Piette E, Daoust R, Denault A. Basic concepts in the use of thoracic and lung ultrasound. Curr Opin Anaesthesiol. 2013; 26:20–30. DOI: 10.1097/ACO.0b013e32835afd40. PMID: 23103845.20. Lichtenstein DA, Mauriat P. Lung ultrasound in the critically ill neonate. Curr Pediatr Rev. 2012; 8:217–23. DOI: 10.2174/157339612802139389. PMID: 23255876. PMCID: PMC3522086.21. Ashton-Cleary DT. Is thoracic ultrasound a viable alternative to conventional imaging in the critical care setting? Br J Anaesth. 2013; 111:152–60. DOI: 10.1093/bja/aet076. PMID: 23585400.22. Trinavarat P, Riccabona M. Potential of ultrasound in the pediatric chest. Eur J Radiol. 2014; 83:1507–18. DOI: 10.1016/j.ejrad.2014.04.011. PMID: 24844730.23. de Graaff JC, Bijker JB, Kappen TH, van Wolfswinkel L, Zuithoff NP, Kalkman CJ. Incidence of intraoperative hypoxemia in children in relation to age. Anesth Analg. 2013; 117:169–75. DOI: 10.1213/ANE.0b013e31829332b5. PMID: 23687233.24. Lichtenstein DA. BLUE-protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill. Chest. 2015; 147:1659–70. DOI: 10.1378/chest.14-1313. PMID: 26033127.25. Díaz-Gómez JL, Renew JR, Ratzlaff RA, Ramakrishna H, Via G, Torp K. Can lung ultrasound be the first-line tool for evaluation of intraoperative hypoxemia? Anesth Analg. 2017; Epub ahead of print. DOI: 10.1213/ANE.0000000000002578.
