Coexistent Actinomycosis and Fungus Ball in the Maxillary Sinus: A Case Report
- Affiliations
-
- 1Department of Otorhinolaryngology-Head & Neck Surgery, Daegu Fatima Hospital, Daegu, Republic of Korea
- 2Department of Pathology, Daegu Fatima Hospital, Daegu, Republic of Korea
- KMID: 2536585
- DOI: http://doi.org/10.18787/jr.2022.00406
Abstract
- Actinomycosis is rarely accompanied by fungus balls. It is difficult to distinguish between actinomycosis and a fungus ball due to their similar clinical and computed tomography scan results. Thus, a meticulous histopathological examination is required for definite diagnosis. We report a case of actinomycosis accompanied by a fungus ball, found incidentally in a patient without rhinologic symptoms. The patient was successfully treated with endoscopic sinus surgery, followed by short-term antibiotic therapy. We suggest that shortterm antibiotic therapy may be more appropriate than long-term antibiotic therapy based on our case study as well as several other studies.
Keyword
Figure
-
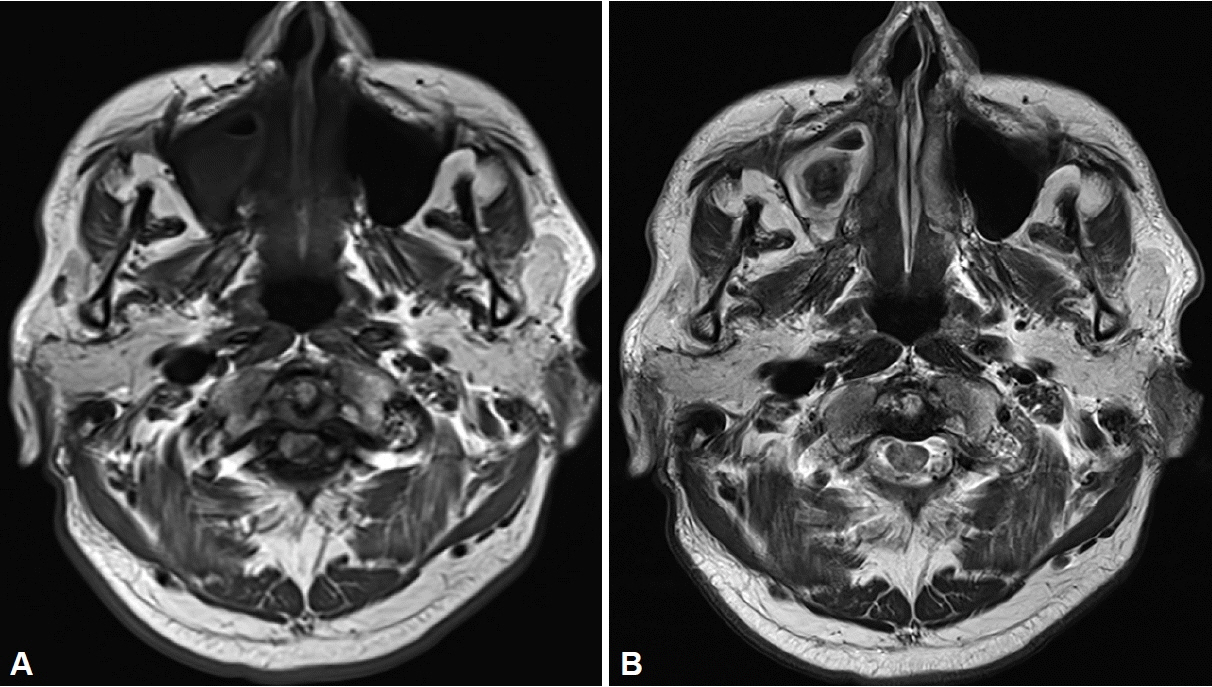
Fig. 1. Magnetic resonance imaging (MRI). A: T1-weighted MRI displaying isointense signal in the right maxillary sinus. B: T2-weighted MRI demonstrating a hypointense signal, called signal voiding, in the right maxillary sinus.

Fig. 2. Computed tomography scan showing partial opacification, with calcification, in the right maxillary sinus (A: axial, B: coronal).
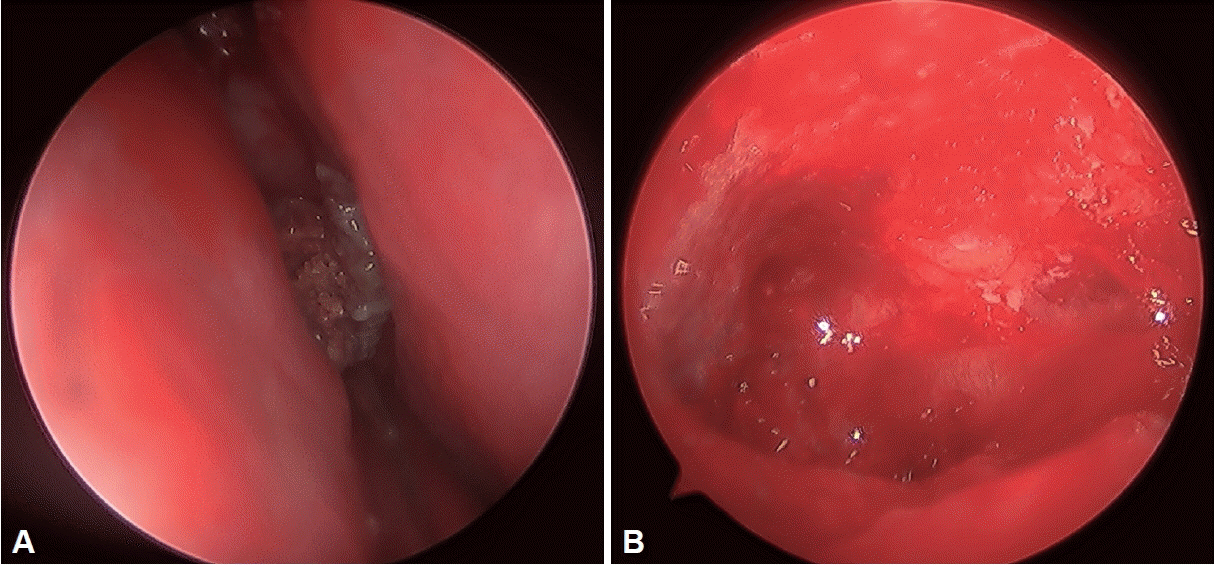
Fig. 3. Intraoperative findings. A: The hard grey and brown lesion is observed in the right middle meatus. B: The severely inflamed mucosa is found in the right maxillary sinus.

Fig. 4. Histopathologic findings. A: Hematoxylin and Eosin staining (×200) showing a sulfur granule surrounded by neutrophilic inflammatory cells (arrowhead) and fungal hyphae (asterisk). B: Gomori methenamine silver statin (×200) revealing thin filamentous rods in the sulfur granule of actinomycosis (arrowhead) and septae branching at a 45° (asterisk), consistent with Aspergillus.
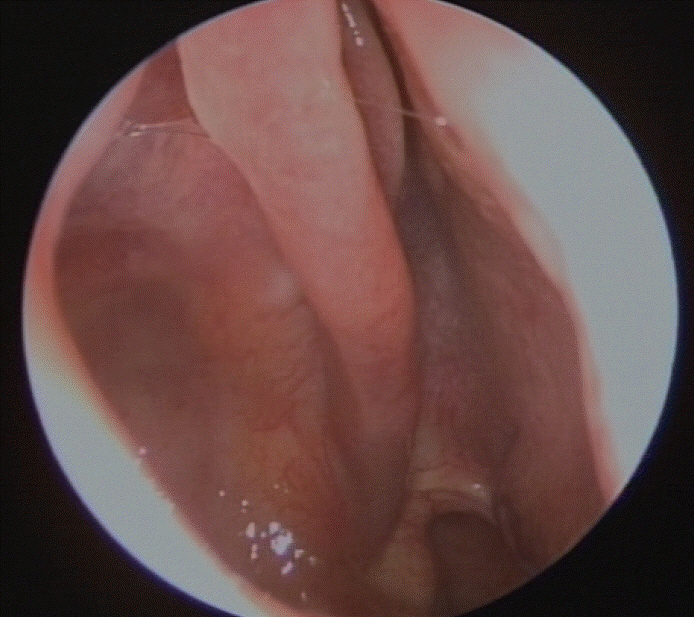
Fig. 5. Postoperatively endoscopic finding showing the healthy mucosa in the right middle meatus. No evidence of recurrence is seen.
Reference
-
References
1. Varghese L, Cherian LM, Varghese GM. Actinomycosis: an unusual cause of maxillary sinusitis. Ear Nose Throat J. 2022; 101(7):433–4.
Article2. Dufour X, Kauffmann-Lacroix C, Ferrie JC, Goujon JM, Rodier MH, Klossek JM. Paranasal sinus fungus ball: epidemiology, clinical features and diagnosis. A retrospective analysis of 173 cases from a single medical center in France, 1989-2002. Med Mycol. 2006; 44(1):61–7.
Article3. Cardoso IC, de Mattos Oliveira F, Hochhegger B, Severo LC. Sphenoid sinus fungus ball by filaments of actinomycetes and Aspergillus fumigatus. Mycopathologia. 2015; 179(5-6):471–3.
Article4. Won HR, Park JH, Kim KS. Simultaneous actinomycosis with aspergillosis in maxillary sinus. Br J Oral Maxillofac Surg. 2013; 51(4):e51–3.
Article5. Bhandarkar AM, Kudva R, Damry K, Radhakrishnan B. Fungus ball in the nasal cavity mimicking a rhinolith. BMJ Case Rep. 2016; 2016:bcr2016215490.
Article6. Woo HJ, Bae CH, Song SY, Choi YS, Kim YD. Actinomycosis of the paranasal sinus. Otolaryngol Head Neck Surg. 2008; 139(3):460–2.
Article7. Sudhakar SS, Ross JJ. Short-term treatment of actinomycosis: two cases and a review. Clin Infect Dis. 2004; 38(3):444–7.
Article8. Grosjean P, Weber R. Fungus balls of the paranasal sinuses: a review. Eur Arch Otorhinolaryngol. 2007; 264(5):461–70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Actinomycosis of the Maxillary Sinus Accompanied with Fungal Ball
- A Case of Supernumerary Tooth within Fungus Ball in the Maxillary Sinus
- Characteristic features of fungus ball in the maxillary sinus and the location of intralesional calcifications on computed tomographic images: A report of 2 cases
- Clinical Characteristics According to the Radiological Classifications of Maxillary Sinus Fungus Ball
- A Case of Fungal Ball Caused by Retained Glass Foreign Body in Maxillary Sinus for 30 Years
