Clinical Characteristics According to the Radiological Classifications of Maxillary Sinus Fungus Ball
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, School of Medicine, Wonkwang University, Iksan, Republic of Korea
- KMID: 2528317
- DOI: http://doi.org/10.18787/jr.2021.00392
Abstract
- Background and Objectives
The purpose of this study was to classify radiological findings of patients diagnosed with maxillary sinus fungus ball and to analyze the differences in surgical approach methods and postoperative results.
Methods
As a retrospective study, we reviewed the medical records of 221 patients (unilateral in 216: bilateral in 5).
Results
On computed tomography (CT), 49% of the lesions had an irregular surface or a protruding part. There was a significant difference in surgical approach according to pneumatization of the maxillary sinus when middle meatal antrostomy (MMA) was performed alone or combined with MMA and inferior meatal antrostomy (IMA) (p=0.042). Extension of a maxillary sinus lesion caused by fungus ball was not associated with stenosis of the MMA (p=0.328).
Conclusion
Diagnosis of maxillary sinus fungus on CT was associated with irregular lesion surface or a protruding calcification. In patients with fungus ball of the maxillary sinus, the more severe is the maxillary sinus pneumatization, the larger is the extent of IMA needed.
Keyword
Figure
-
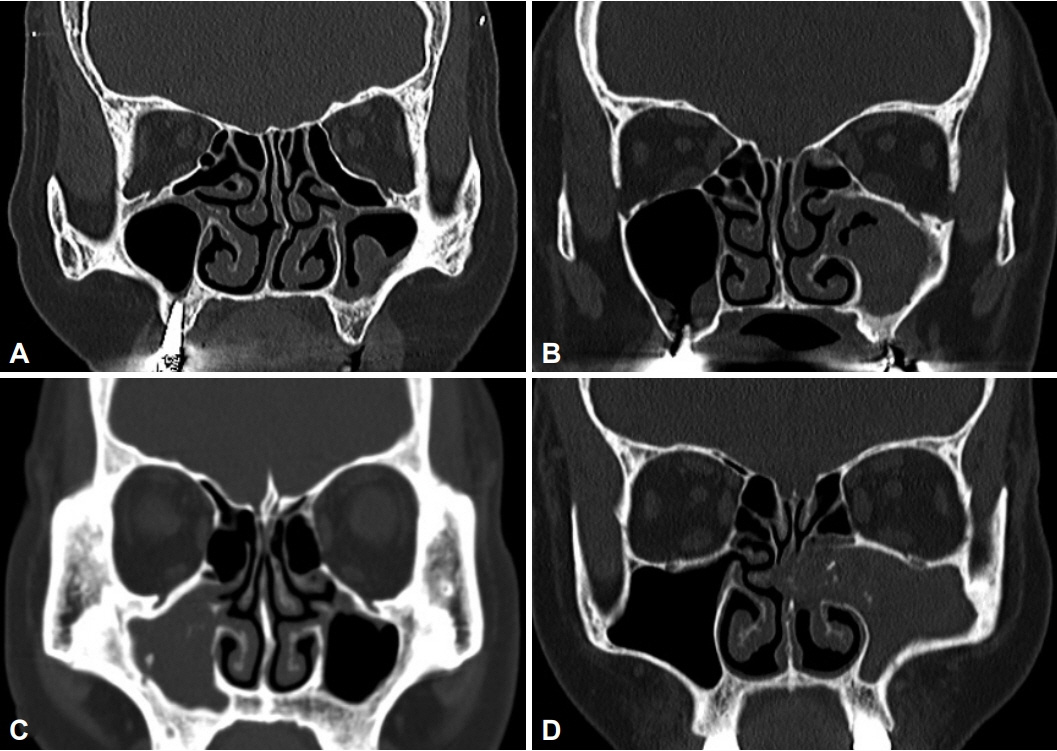
Fig. 1. Computed tomographic findings of maxillary sinus fungus ball. Grade I shows a haziness less than 50% of the whole maxillary sinus with the irregular mucosal surface or a protruding lesion (A). Grade II shows a haziness more than 50% of the whole maxillary sinus and it is not the whole haziness, the mucosal part has the irregular surface or a protruding lesion (B). Grade III shows total haziness of maxillary sinus without mass effect (C). Grade IV shows total haziness of maxillary sinus with mass effect (D).
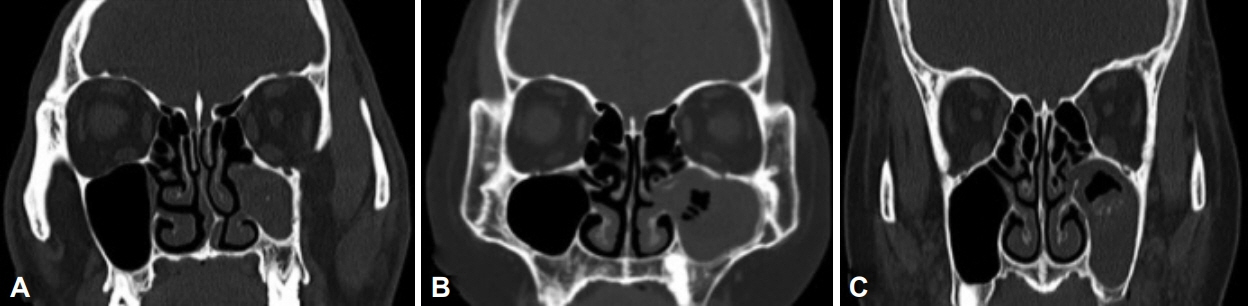
Fig. 2. Computed tomographic findings of maxillary sinus pneumatization. Grade I shows maxillary sinus pneumatization limited above the nasal floor level (A). Grade II shows maxillary sinus pneumatization limited to the nasal floor level (B). Grade III shows maxillary sinus pneumatization extended below the nasal floor level (C).
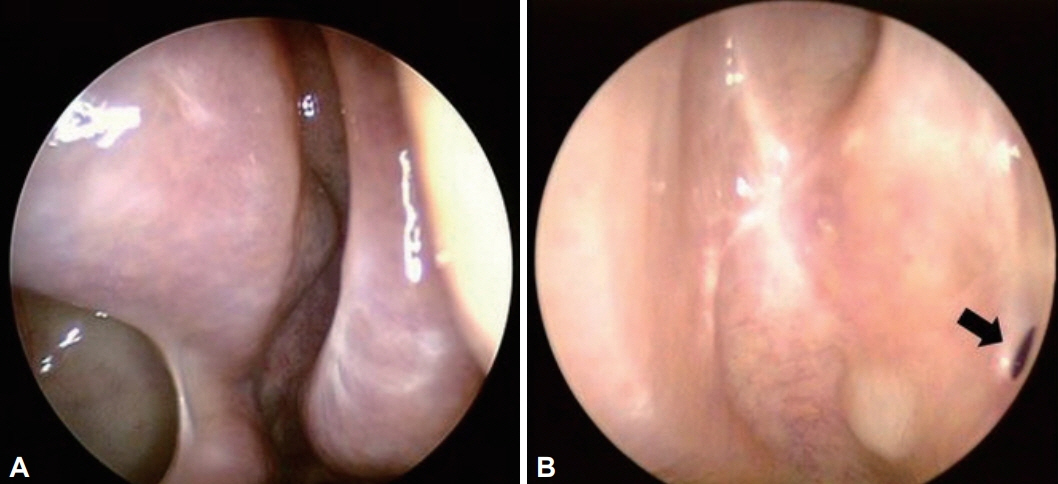
Fig. 3. Postoperative findings of well-opened (A) and stenotic (B) middle meatal antrostomy site (arrow: stenotic middle meatal antrostomy site).
Reference
-
References
1. Ferguson BJ. Fungus balls of the paranasal sinuses. Otolaryngol Clin North Am. 2000; 33(2):389–98.
Article2. Broglie MA. Tinguely M, Holzman D. How to diagnose sinus fungus balls in the paranasal sinus? An analysis of an institution’s cases from January 1999 to December 2006. Rhinology. 2009; 47(4):379–84.3. Nicolai P, Lombardi D, Tomenzoli D, Vilaret AB, Piccioni M, Mensi M, et al. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009; 119(11):2275–9.
Article4. Kim JS, So SS, Kwon SH. The increasing incidence of paranasal sinus fungus ball: a retrospective cohort study in two hundred forty-five patients for fifteen years. Clin Otolaryngol. 2017; 42(1):175–9.
Article5. Cha H, Song Y, Bae YJ, Won TB, Kim J, Cho S, et al. Clinical characteristics other than intralesional hyperdensity may increase the preoperative diagnostic accuracy of maxillary sinus fungal ball. Clin Exp Otorhinolaryngol. 2020; 13(2):157–63.
Article6. Ju Y, Byun K, Ahn J, Choi K, Mo J, Chung Y. Comparison of postoperative results according to fungus ball extension in maxillary sinus. Korean J Otorhinolaryngol-Head Neck Surg. 2021; 64(1):13–8.
Article7. Sawatsubashi M, Murakami D, Umezaki T, Komune S. Endonasal endoscopic surgery with combined middle and inferior meatal antrostomies for fungal maxillary sinusitis. J Laryngol Otol. 2015; 129 Suppl 2:S52–5.
Article8. Choi Y, Kim B, Kang S, Yu MS. Feasibility of minimal inferior meatal antrostomy and fiber-optic sinus exam for fungal sinusitis. Am J Rhinol Allergy. 2019; 33(6):634–9.
Article9. Dufour X, Kauffmann-Lacroix C, Ferrie JC, Goujon JM, Rodier MH, Klossek JM. Paranasal sinus fungus ball: epidemiology, clinical features and diagnosis. A retrospective analysis of 173 cases from a single medical center in France, 1989-2002. Med Mycol. 2006; 44(1):61–7.
Article10. Seo YJ, Kim J, Kim K, Lee JG, Kim CH, Yoon JH. Radiologic characteristics of sinonasal fungus ball: an analysis of 119 cases. Acta Radiol. 2011; 52(7):790–5.
Article11. Kim HJ, Choi JH, Lee JY. Evaluation of recurrent maxillary sinusitis due to middle meatal antrostomy site stenosis. Ann Otol Rhnol Laryngol. 2020; 129(10):964–8.
Article12. Lee JH. A clinical analysis of postoperative cheek cyst: 10-year experience. J Clin Otolaryngol Head Neck Surg. 2012; 23(1):79–84.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Supernumerary Tooth within Fungus Ball in the Maxillary Sinus
- Characteristic features of fungus ball in the maxillary sinus and the location of intralesional calcifications on computed tomographic images: A report of 2 cases
- Comparative Study of Fungus Ball and Chronic Bacterial Sinusitis
- Secondary Fungus Ball Caused by a Retained Foreign Body in Maxillary Sinus
- A Case of Fungal Ball Caused by Retained Glass Foreign Body in Maxillary Sinus for 30 Years
