Efficacy of geriatric multidisciplinary oncology clinic in the surgical treatment decision-making process for frail elderly patients with colorectal cancer
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Division of Hematology and Medical Oncology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 3Department of Radiation Oncology, Seoul National University Bundang Hospital, Seongnam, Korea
- 4Division of Geriatrics, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- KMID: 2532929
- DOI: http://doi.org/10.4174/astr.2022.103.3.169
Abstract
- Purpose
Multidisciplinary care has become a cornerstone of colorectal cancer management. To evaluate the clinical efficacy of a geriatric multidisciplinary oncology clinic (GMOC), we analyzed the surgical treatment decision-making process and outcomes.
Methods
This retrospective single-center study reviewed the data of patients aged ≥65 years who participated in the GMOC at a tertiary referral hospital between 2015 and 2021. The clinical adherence rate, comprehensive geriatric assessment, and a multidimensional frailty score (MFS) were obtained. The groups that were recommended and not recommended for surgery were compared, analyzing the factors impacting the decision and 1-year survival outcomes. Furthermore, the postoperative complications of patients who underwent surgery were evaluated.
Results
A total of 165 patients visited the GMOC, and 74 had colorectal cancer (mean age, 85.5 years [range, 81.2–89.0 years]). Among patients with systemic disease (n = 31), 7 were recommended for surgery, and 5 underwent surgery. Among patients with locoregional disease (n = 43), 18 were recommended for surgery, and 12 underwent surgery. Patients recommended and not recommended for surgery had significantly different activities of daily living (ADL) (P = 0.024), instrumental ADL (P = 0.001), Mini-Mental State Examination (P = 0.014), delirium risk (P = 0.039), and MFS (P = 0.001). There was no difference in the 1-year overall survival between the 2 groups (P = 0.980). Of the 17 patients who underwent surgery, the median (interquartile range) of operation time was 165.0 minutes (120.0–270.0 minutes); hospital stay, 7.0 days (6.0–8.0 days); and 3 patients had wound complications.
Conclusion
Proper counseling of patients through the GMOC could lead to appropriate management and favorable outcomes.
Keyword
Figure
-
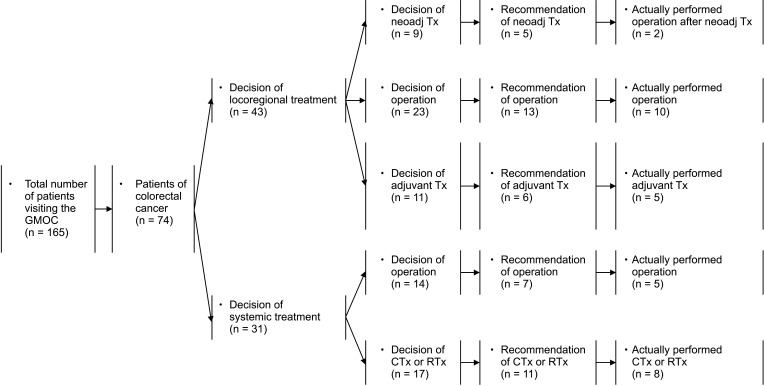
Fig. 1 Flow of clinical decision process. In all patients, the clinical adherence rate to the medical recommendation was 40.5% (30 of 74). GMOC, geriatric multidisciplinary oncology clinic; neoadj, neoadjuvant; Tx, therapy; CTx, chemotherapy; RTx, radiotherapy.
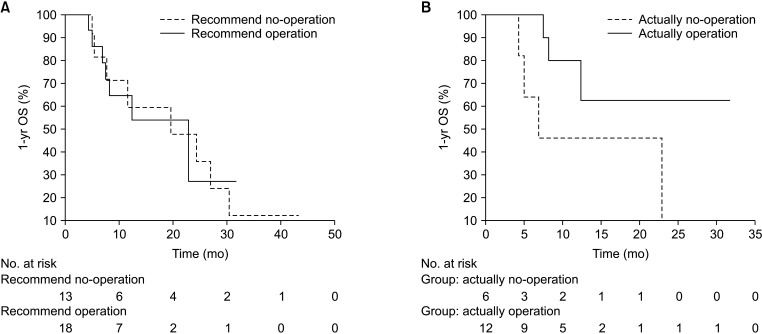
Fig. 2 The overall survival (OS) of 1 year in recommended and actual operation groups. (A) According to recommended for operation (n = 32). (B) According to actual operation (n = 18).
Cited by 2 articles
-
Weighing the benefits of lymphadenectomy in early-stage colorectal cancer
Seung Min Baik, Ryung-Ah Lee
Ann Surg Treat Res. 2023;105(5):245-251. doi: 10.4174/astr.2023.105.5.245.National cancer screening program for colorectal cancer in Korea
Seung Min Baik, Ryung-Ah Lee
Ann Surg Treat Res. 2023;105(6):333-340. doi: 10.4174/astr.2023.105.6.333.
Reference
-
1. Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al. Cancer today: global cancer observatory [Internet]. Lyon: International Agency for Research on Cancer;World Health Organization;2022. cited 2022 Mar 9. Available from: https://gco.iarc.fr/today .2. Orimo H, Ito H, Suzuki T, Araki A, Hosoi T, Sawabe M. Reviewing the definition of “elderly”. Geriatr Gerontol Int. 2006; 6:149–158.
Article3. Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004; 59:255–263. PMID: 15031310.
Article4. Couwenberg AM, de Beer FS, Intven MP, Burbach JP, Smits AB, Consten EC, et al. The impact of postoperative complications on health-related quality of life in older patients with rectal cancer; a prospective cohort study. J Geriatr Oncol. 2018; 9:102–109. PMID: 29032962.
Article5. Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010; 210:901–908. PMID: 20510798.
Article6. Hamaker ME, Jonker JM, de Rooij SE, Vos AG, Smorenburg CH, van Munster BC. Frailty screening methods for predicting outcome of a comprehensive geriatric assessment in elderly patients with cancer: a systematic review. Lancet Oncol. 2012; 13:e437–e444. PMID: 23026829.
Article7. Kim KI, Park KH, Koo KH, Han HS, Kim CH. Comprehensive geriatric assessment can predict postoperative morbidity and mortality in elderly patients undergoing elective surgery. Arch Gerontol Geriatr. 2013; 56:507–512. PMID: 23246499.
Article8. Kim SW, Han HS, Jung HW, Kim KI, Hwang DW, Kang SB, et al. Multidimensional frailty score for the prediction of postoperative mortality risk. JAMA Surg. 2014; 149:633–640. PMID: 24804971.
Article9. Presley CJ, Krok-Schoen JL, Wall SA, Noonan AM, Jones DC, Folefac E, et al. Implementing a multidisciplinary approach for older adults with cancer: geriatric oncology in practice. BMC Geriatr. 2020; 20:231. PMID: 32631254.
Article10. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987; 40:373–383. PMID: 3558716.
Article11. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965; 14:61–65.12. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969; 9:179–186. PMID: 5349366.
Article13. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999; 15:116–122. PMID: 9990575.
Article14. American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012; 60:616–631. PMID: 22376048.15. Lee DY, Lee JH, Ju YS, Lee KU, Kim KW, Jhoo JH, et al. The prevalence of dementia in older people in an urban population of Korea: the Seoul study. J Am Geriatr Soc. 2002; 50:1233–1239. PMID: 12133018.
Article16. Bae JN, Cho MJ. Development of the Korean version of the Geriatric Depression Scale and its short form among elderly psychiatric patients. J Psychosom Res. 2004; 57:297–305. PMID: 15507257.
Article17. Gaudreau JD, Gagnon P, Harel F, Tremblay A, Roy MA. Fast, systematic, and continuous delirium assessment in hospitalized patients: the nursing delirium screening scale. J Pain Symptom Manage. 2005; 29:368–375. PMID: 15857740.
Article18. Mohanty S, Rosenthal RA, Russell MM, Neuman MD, Ko CY, Esnaola NF. Optimal perioperative management of the geriatric patient: a best practices guideline from the American College of Surgeons NSQIP and the American Geriatrics Society. J Am Coll Surg. 2016; 222:930–947. PMID: 27049783.
Article19. Mohile SG, Dale W, Somerfield MR, Schonberg MA, Boyd CM, Burhenn PS, et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO Guideline for Geriatric Oncology. J Clin Oncol. 2018; 36:2326–2347. PMID: 29782209.
Article20. National Comprehensive Cancer Network (NCCN). Older adult oncology (version 1.2022) [Internet]. Plymouth Meeting, PA: NCCN;2022. cited 2022 Apr 24. Available from: https://www.nccn.org/professionals/physician_gls/pdf/senior.pdf .21. Zietlow K, McDonald SR, Sloane R, Browndyke J, Lagoo-Deenadayalan S, Heflin MT. Preoperative cognitive impairment as a predictor of postoperative outcomes in a collaborative care model. J Am Geriatr Soc. 2018; 66:584–589. PMID: 29332302.
Article22. Kristjansson SR, Jordhøy MS, Nesbakken A, Skovlund E, Bakka A, Johannessen HO, et al. Which elements of a comprehensive geriatric assessment (CGA) predict post-operative complications and early mortality after colorectal cancer surgery? J Geriatr Oncol. 2010; 1:57–65.
Article23. Stegmann ME, Festen S, Brandenbarg D, Schuling J, van Leeuwen B, de Graeff P, et al. Using the Outcome Prioritization Tool (OPT) to assess the preferences of older patients in clinical decision-making: a review. Maturitas. 2019; 128:49–52. PMID: 31561823.
Article24. Jung SM, Hong YS, Kim TW, Park JH, Kim JH, Park SH, et al. Impact of a multidisciplinary team approach for managing advanced and recurrent colorectal cancer. World J Surg. 2018; 42:2227–2233. PMID: 29282505.
Article
