Genomic Sequencing for Bladder Urothelial Carcinoma and Its Clinical Implications for Immunotherapy
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2531335
- DOI: http://doi.org/10.4143/crt.2021.854
Abstract
- Purpose
This study aimed to explore the genomic and transcriptomic landscape of bladder cancer (BC) and its implication for treatment with an immune checkpoint inhibitor (ICI).
Materials and Methods
We analyzed whole-exome and -transcriptome sequences of tumor samples from 64 BC patients who underwent surgical resection with either transurethral resection or radical cystectomy. For exploratory purposes, programmed death-ligand 1 (PD-L1) expression was evaluated in a subset of patients (n=57) including those treated with ICI (n=8).
Results
We identified frequent molecular dysregulations in chromatin regulatory genes (KDM6A, ARID1A, MLL2, and STAG2) and recurrent copy number alterations. Thirty-five samples (54.7%) were PD-L1–positive (PD-L1 combined positive score ≥ 1) with a significantly higher exonic tumor mutational burden (TMB) compared to PD-L1–negative BC samples (p=0.010). We observed that various immune-responsive pathways, including the PD-L1 signaling pathway, were enriched significantly in PD-L1–positive BCs. Interestingly, genes in the CTLA4 pathway were enriched significantly in PD-L1–positive BC as well. Among eight patients who received ICI, progressive disease was confirmed in one patient, whose tumor had low exonic TMB, negative PD-L1 status, and a relatively colder microenvironment.
Conclusion
Gaining new insights into the molecular landscape of BC will improve treatment strategies. Our analysis suggests a rationale for studying dual checkpoint inhibition against BC.
Keyword
Figure
-
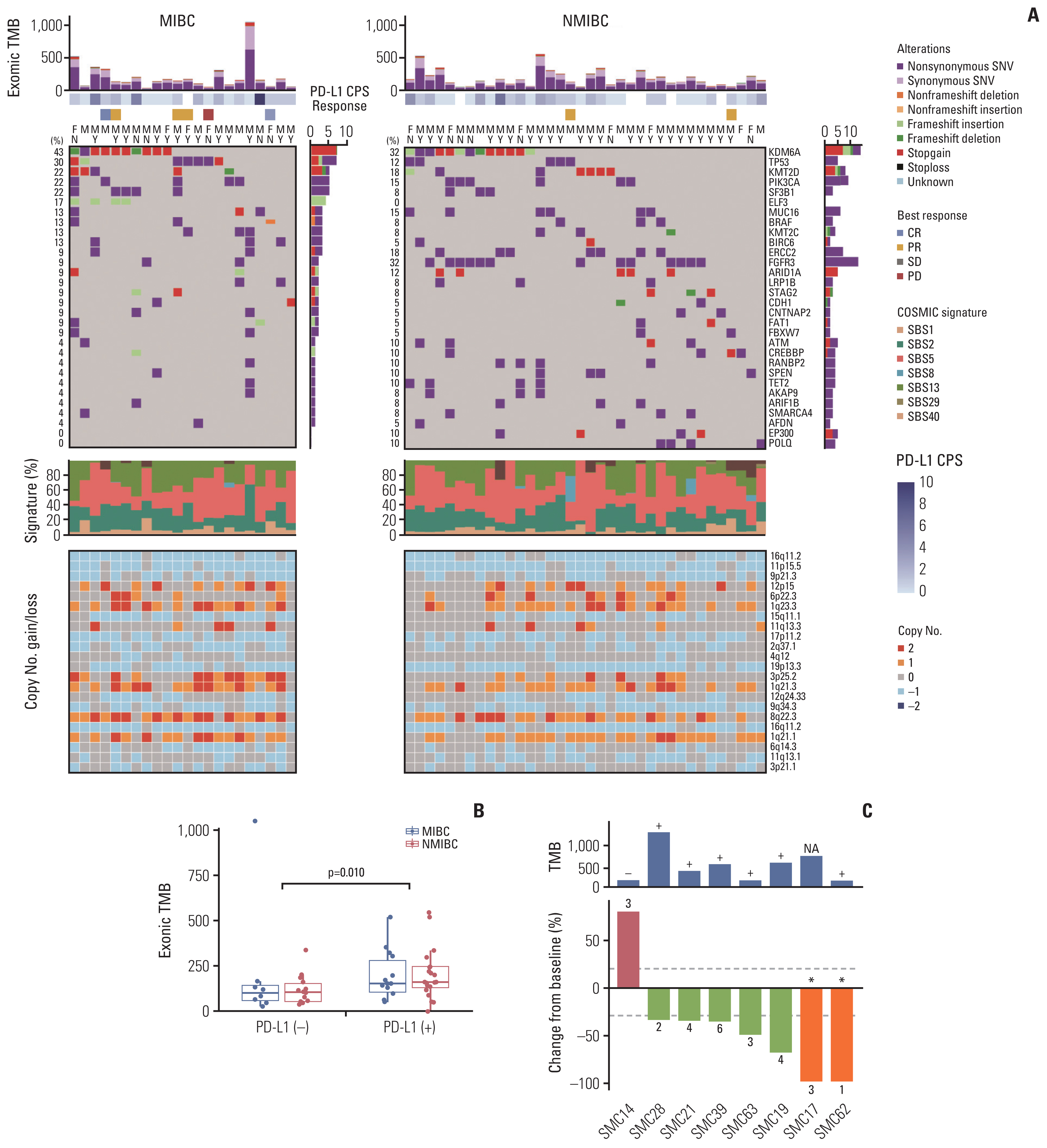
Fig. 1 The landscape of somatic mutations in bladder cancer and therapeutic efficacy of immunotherapy in a subset of patients. (A) Exonic somatic mutational landscape for 63 primary tumors. Top to bottom: synonymous and non-synonymous somatic tumor mutational burden (TMB) in the exome, programmed death-ligand 1 (PD-L1) combined positive score, response to an immune checkpoint inhibitor, sex, smoking history, somatic single-nucleotide variations and indels for 30 most frequently mutated genes, normalized activity of seven mutational signatures, and copy number alterations for significantly amplified (red) or deleted (blue) cytobands with q-value < 0.001 determined by the Genomic Identification of Significant Targets in Cancer (GISTC) algorithm. (B) The differences of exonic TMB between PD-L1–positive and PD-L1–negative muscle-invasive bladder cancer (MIBC) and non-muscle-invasive bladder cancer (NMIBC). The statistical significance of the differences was estimated by the Wilcoxon signed-rank test. (C) The treatment outcome of eight patients who received immunotherapy. (Upper) A bar plot illustrating patient exonic TMB and PD-L1–positivity (+, PD-L1–positive BC; −, PD-L1–negative BC). (Lower) Waterfall plot of responses to immunotherapy in a subset of eight patients. The Samsung Medical Center (SMC) represents each patient’s identification number. The Y-axis represents the percentage of maximum tumor reduction assessed according to Response Evaluation Criteria in Solid Tumor 1.1 criteria. The upper and lower dotted lines represent 20% tumor expansion and 30% tumor reduction, respectively, which define progressive disease (PD) and partial response (PR). Two patients marked with an asterisk (*) had complete response (CR) after treatment with immune checkpoint inhibitor plus chemotherapy combination. CPS, combined positive score; F, female; M, male; N, non-smoker; SBS, single-base substitution; SD, stable disease; SNV, single-nucleotide variant; Y, smoker.
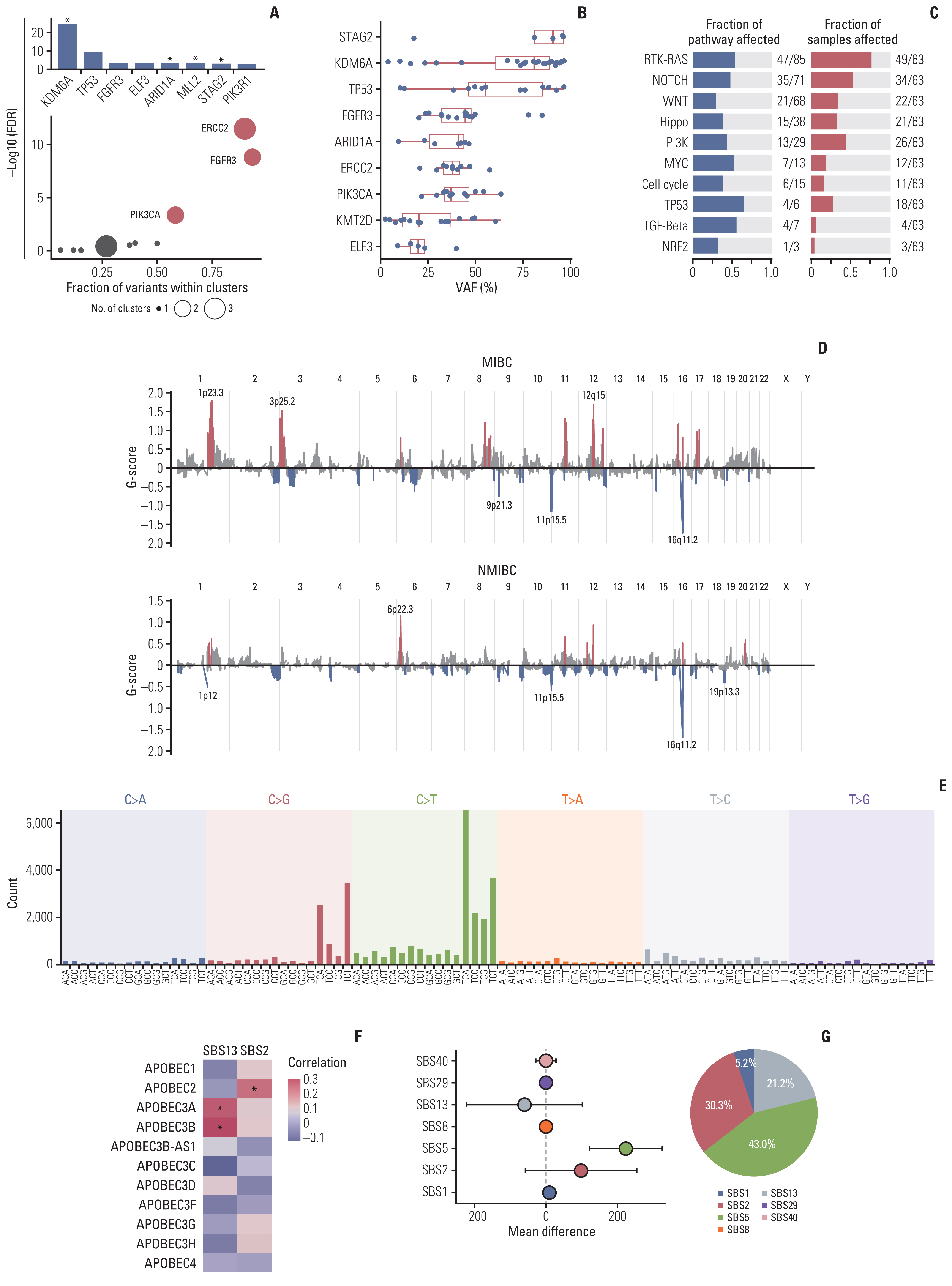
Fig. 2 Driver mutations, copy number alterations, and mutational signature of bladder cancer. (A) Putative driver mutations in bladder cancer (BC), identified using MutSigCV (upper) and oncodriveCLUST (lower) algorithms. The oncodriveCLUST algorithm is based on enrichment at few specific loci of most variants in cancer-causing genes. This method takes advantage of such a position to identify cancer genes. A scatter plot in the lower panel illustrates the size of the points proportional to the number of clusters found in the gene. The X-axis shows the number of mutations (or fraction of mutations) observed in these clusters. FDR, false discovery rate. (B) The variant-allele frequency (VAF) distribution of the putative driver genes in our cohort. Dots represent a VAF of each driver mutation identified in a sample. The median, first, and third quartiles of the VAF distribution are indicated by a red-colored box. (C) Enrichment of known oncogenic signaling pathways in The Cancer Genome Atlas cohorts. Fractions of the affected pathways are demonstrated on the left, while the fraction of affected samples is shown on the right. (D) A genomic plot with segments highlighting significant amplification (red, above the horizontal line) and deletion (blue, below the horizontal line) regions. The G-score was assigned using the Genomic Identification of Significant Targets in Cancer (GISTIC) algorithm considering the amplitude of the aberration and the frequency of its occurrence across samples. False discovery rate q-values were calculated for the aberrant regions, and regions with a q-value less than 0.10 were considered statistically significant. MIBC, muscle invasive bladder cancer; NMIBC, non–muscle invasive bladder cancer. (E) The signatures of exonic somatic single-base substitutions (SBSs) delineated by COSMIC signatures. (F) The correlation between the proportion of SBS2, SBS3, and the mRNA expression of APOBEC genes. The correlation was estimated by the Pearson correlation coefficient. Statistically significant correlations are annotated by an asterisk (*). (G) The enrichment of each SBS in smokers. We compared the absolute number of SBS attributed to each signature between smokers and non-smokers. The statistical significance was estimated using Student’s t test.

Fig. 3 mRNA expression of programmed death-ligand 1 (PD-L1)–positive and PD-L1–negative bladder cancer (BC). (A) Heatmap of Gene Set Variation Analysis (GSVA) scores across BC samples. Top to bottom: an unsupervised clustering of samples, combined positive immunohistochemistry scoring of PD-L1, the best response to immunotherapy, a heatmap demonstrating enrichment score-estimated GSVA. Pathways involved in the immune response are annotated on the right. (B) A volcano plot showing differentially activated pathways between PD-L1–positive and PD-L1–negative BCs. (C) The correlations between enrichment score of programmed death-1 (PD-1) (y-axis) signaling and cytotoxic T-lymphocyte antigen 4 (CTLA-4) (x-axis) signaling pathways. (D) Average enrichment score of immune-related pathways in PD-L1–negative and PD-L1–positive BC. (E) A scatter plot simultaneously demonstrating the tumor mutational burden (TMB, x-axis), averaged immune score (x-axis), and PD-L1 positivity (size). Each dot represents a case, with the size of the dot representing PD-L1 positivity. The x-axis and y-axis correspond to the TMB and averaged immune score, respectively. Two patients who experienced complete response (CR) are indicated by an asterisk (*). CPS, combined positive score; PD, progressive disease; PR, partial response; SD, stable disease.
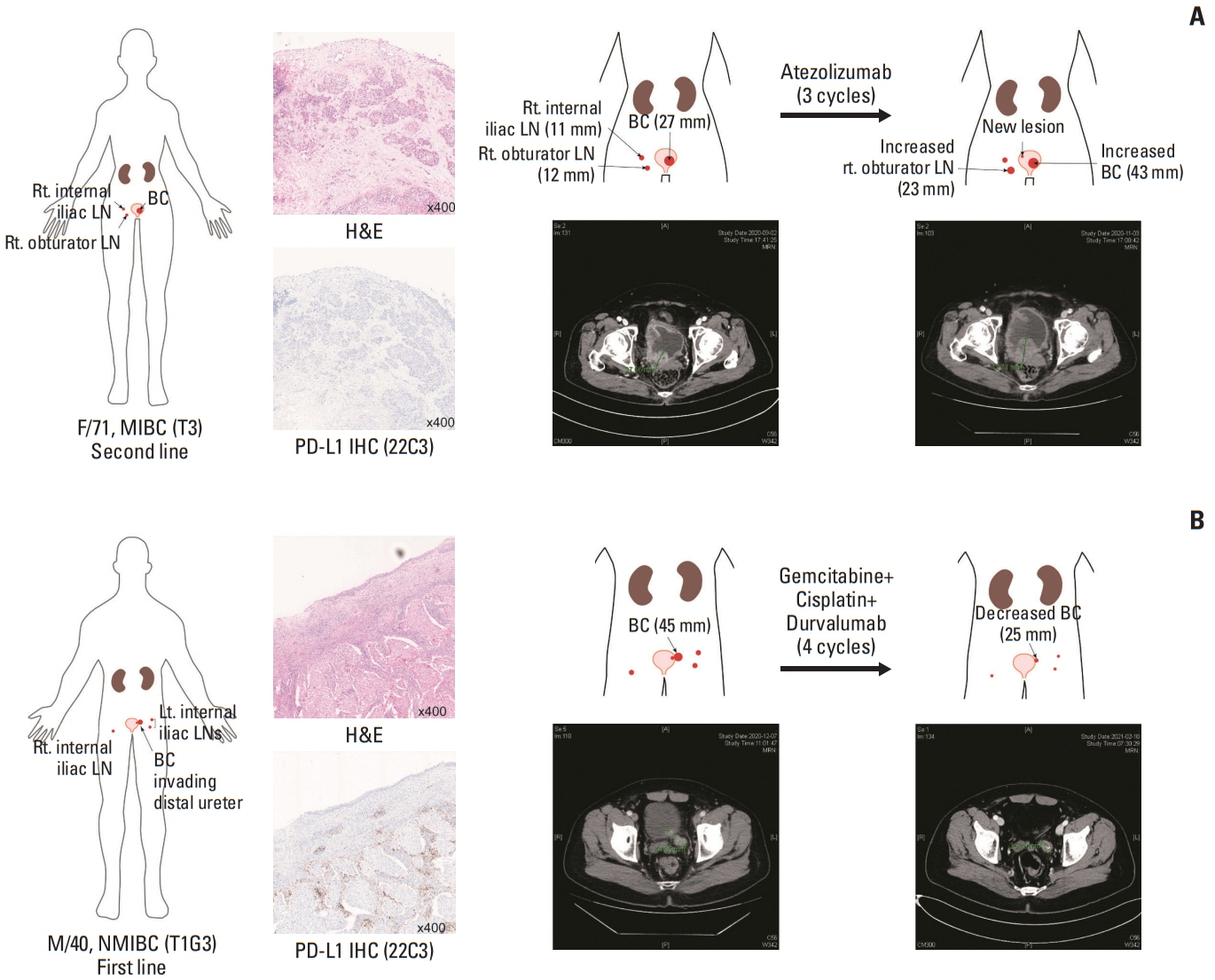
Fig. 4 Two representative cases of progressive disease and partial response during treatment with immune checkpoint inhibitors. (A) A 71-year-old female (SMC14) had muscle-invasive bladder cancer (MIBC) at the left lateral wall of the bladder. The tumor specimen showed negative programmed death-ligand 1 (PD-L1) staining (middle) and had low tumor mutational burden (Fig. 1C). Initially, the tumor did not respond to two cycles of gemcitabine plus cisplatin. She received three additional cycles of palliative atezolizumab (right). However, the primary mass and metastatic lymph nodes increased in size, and a new lesion was identified at the left side of the trigone. (B) A 40-year-old male (SMC19) with T1G3 bladder cancer (BC) had a primary mass at the left lateral bladder wall and several lymph node (LN) metastases. The primary bladder mass was PD-L1–positive (middle) and responded dramatically to four cycles of durvalumab in combination with gemcitabine and cisplatin. IHC, immunohistochemistry; Lt., left; NMIBC, non–muscle invasive bladder cancer; Rt., right.
Reference
-
References
1. Witjes JA, Bruins HM, Cathomas R, Comperat EM, Cowan NC, Gakis G, et al. European Association of Urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol. 2021; 79:82–104.2. Patel VG, Oh WK, Galsky MD. Treatment of muscle-invasive and advanced bladder cancer in 2020. CA Cancer J Clin. 2020; 70:404–23.
Article3. Lawrence MS, Stojanov P, Polak P, Kryukov GV, Cibulskis K, Sivachenko A, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013; 499:214–8.
Article4. Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV, et al. Signatures of mutational processes in human cancer. Nature. 2013; 500:415–21.5. Aggen DH, Drake CG. Biomarkers for immunotherapy in bladder cancer: a moving target. J Immunother Cancer. 2017; 5:94.
Article6. Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature. 2014; 507:315–22.7. Robertson AG, Kim J, Al-Ahmadie H, Bellmunt J, Guo G, Cherniack AD, et al. Comprehensive molecular characterization of muscle-invasive bladder cancer. Cell. 2017; 171:540–56.8. Kim ST, Cristescu R, Bass AJ, Kim KM, Odegaard JI, Kim K, et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat Med. 2018; 24:1449–58.
Article9. Yarchoan M, Albacker LA, Hopkins AC, Montesion M, Murugesan K, Vithayathil TT, et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight. 2019; 4:e126908.
Article10. Lenis AT, Lec PM, Chamie K, Mshs MD. Bladder cancer: a review. JAMA. 2020; 324:1980–91.11. Gondkar K, Patel K, Krishnappa S, Patil A, Nair B, Sundaram GM, et al. E74 like ETS transcription factor 3 (ELF3) is a negative regulator of epithelial-mesenchymal transition in bladder carcinoma. Cancer Biomark. 2019; 25:223–32.
Article12. Gui Y, Guo G, Huang Y, Hu X, Tang A, Gao S, et al. Frequent mutations of chromatin remodeling genes in transitional cell carcinoma of the bladder. Nat Genet. 2011; 43:875–8.
Article13. Tamborero D, Gonzalez-Perez A, Lopez-Bigas N. OncodriveCLUST: exploiting the positional clustering of somatic mutations to identify cancer genes. Bioinformatics. 2013; 29:2238–44.
Article14. Sanchez-Vega F, Mina M, Armenia J, Chatila WK, Luna A, La KC, et al. Oncogenic signaling pathways in the Cancer Genome Atlas. Cell. 2018; 173:321–37.15. Alexandrov LB, Kim J, Haradhvala NJ, Huang MN, Tian Ng AW, Wu Y, et al. The repertoire of mutational signatures in human cancer. Nature. 2020; 578:94–101.
Article16. Powles T, van der Heijden MS, Castellano D, Galsky MD, Loriot Y, Petrylak DP, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020; 21:1574–88.17. van Dijk N, Gil-Jimenez A, Silina K, Hendricksen K, Smit LA, de Feijter JM, et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: the NABUCCO trial. Nat Med. 2020; 26:1839–44.
Article18. Hedegaard J, Lamy P, Nordentoft I, Algaba F, Hoyer S, Ulhoi BP, et al. Comprehensive transcriptional analysis of early-stage urothelial carcinoma. Cancer Cell. 2016; 30:27–42.
Article19. Hurst CD, Alder O, Platt FM, Droop A, Stead LF, Burns JE, et al. Genomic subtypes of non-invasive bladder cancer with distinct metabolic profile and female gender bias in KDM6A mutation frequency. Cancer Cell. 2017; 32:701–15.
Article20. Gajewski TF. The next hurdle in cancer immunotherapy: overcoming the non-T-cell-inflamed tumor microenvironment. Semin Oncol. 2015; 42:663–71.
Article21. Sweis RF, Spranger S, Bao R, Paner GP, Stadler WM, Steinberg G, et al. Molecular drivers of the non-T-cell-inflamed tumor microenvironment in urothelial bladder cancer. Cancer Immunol Res. 2016; 4:563–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tuberculous Prostatic Abscess Following Intravesical Bacillus Calmette-Guerin Instillation
- Seminal Vesicle Involvement by Urothelial Carcinoma in Situ of the Bladder with Mucosal Spread Pattern: A Case Report
- The Development of Antibody-Drug Conjugates for Urothelial Carcinoma Treatment
- High-Grade Urothelial Carcinoma of the Bladder in a Child
- Urothelial Carcinoma in a 17-year-old Boy
