High-Resolution Probe-Based Confocal Laser Endomicroscopy for Diagnosing Biliary Diseases
- Affiliations
-
- 1Department of Gastroenterology, Aichi Cancer Center Hospital, Nagoya, Japan
- 2Department of Gastroenterology, Tottori University Hospital, Yonago, Japan
- KMID: 2522716
- DOI: http://doi.org/10.5946/ce.2020.191
Abstract
- Probe-based confocal laser endomicroscopy is an endoscopic technique that enables in vivo histological evaluation using fluorescent pigment. The ability to diagnostically differentiate between benign and malignant biliary disease using the “CholangioFlexTM”, a dedicated biliary device, has been reported. However, the Miami and Paris classifications, used as diagnostic criteria, mainly evaluate findings in the submucosa, and visualizing the epithelium as the main site of lesions remains difficult. To address this problem, we verified the imaging findings and diagnostic ability of three types of probes: CholangioFlexTM, GastroFlexTM, and AlveoFlexTM. With GastroFlexTM, the clear mucosal epithelium was observed, and differential diagnoses as benign/malignant could be made based on epithelial findings. GastroFlexTM may be a good first-choice probe for probe-based confocal laser endomicroscopy of biliary diseases, and a new diagnostic classification based on bile duct epithelial findings may provide useful criteria independent of the Miami or Paris classifications.
Keyword
Figure
-
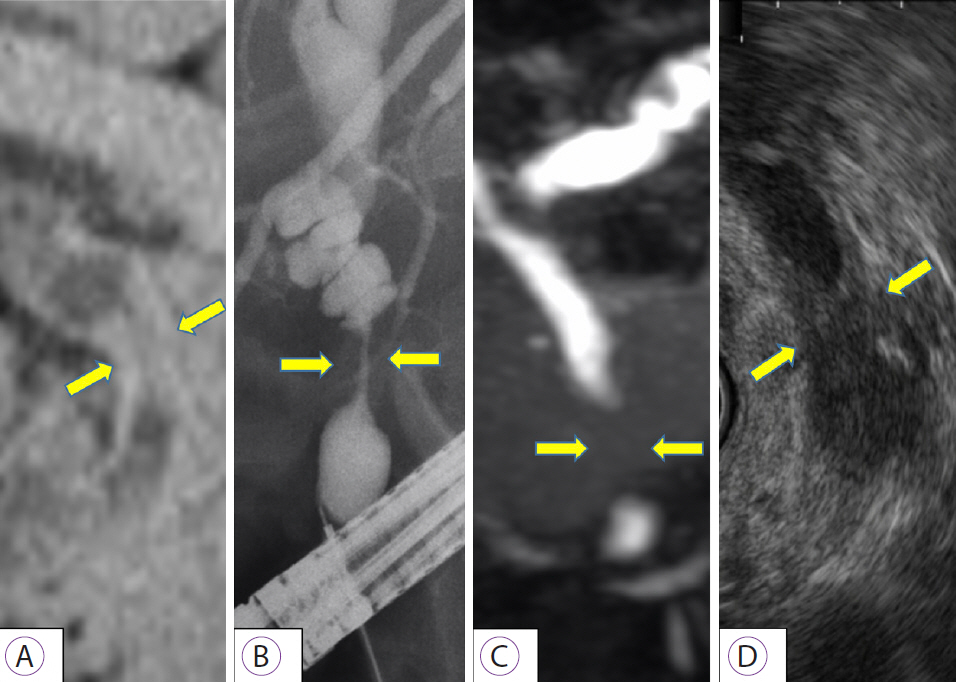
Fig. 1. Imaging findings in bile duct cancer. (A) Computed tomography; (B) endoscopic retrograde cholangiopancreatography; (C) magnetic resonance cholangiopancreatography; (D) endoscopic ultrasonography. Various images show distal bile duct stenosis (yellow arrow) caused by irregular bilateral wall thickness.

Fig. 2. Representative probe-based confocal laser endomicroscopy (pCLE) images of bile duct cancer. Malignant findings, based on the Miami classification, on pCLE with 3 types of probes produced by Mauna Kea Technologies (Paris, France) ((A-C) GastroFlexTM, (D, E) CholangioFlexTM, (F) AlveoFlexTM) are as follows. (A) Thick white bands; (B) dark clumps; (C) epithelial structure; (D) thick dark bands; (E) dark clumps; (F) dark clumps.
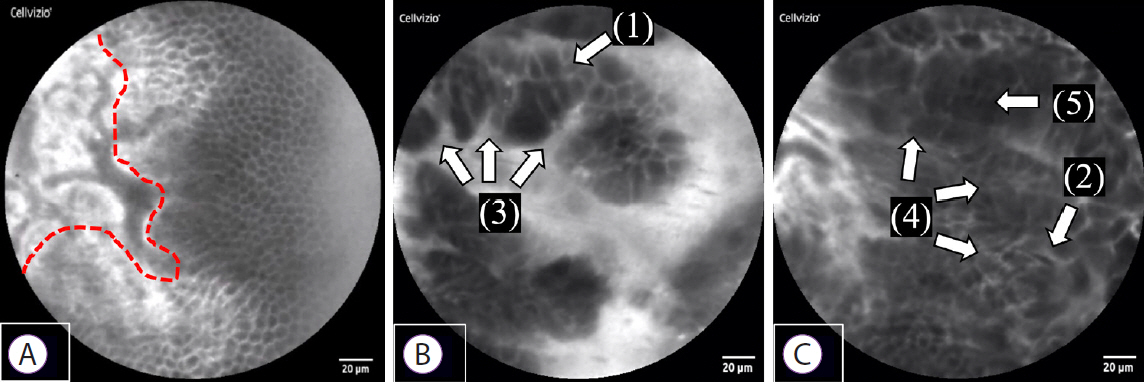
Fig. 3. Normal and malignant findings in epithelial structures. (A) Normal bile duct: a sheet-like monolayer of uniform epithelial cells is arrayed on the right side, and a collagen fiber network in the submucosa is presented on the left side (the red dotted line represents the border). (B, C) Bile duct cancer: (1) Each cell is heterogeneous, and the cells differ in size: cell size difference, (2) Epithelial cells appear to overlap: cell overlap, (3) Irregularity of cell clumps: irregular edges of cell clumps, (4) Irregular and complex epithelial cell composition: irregular structure, (5) The nucleus and cytoplasm cannot be distinguished as the entire cell appears dark: dark epithelium.
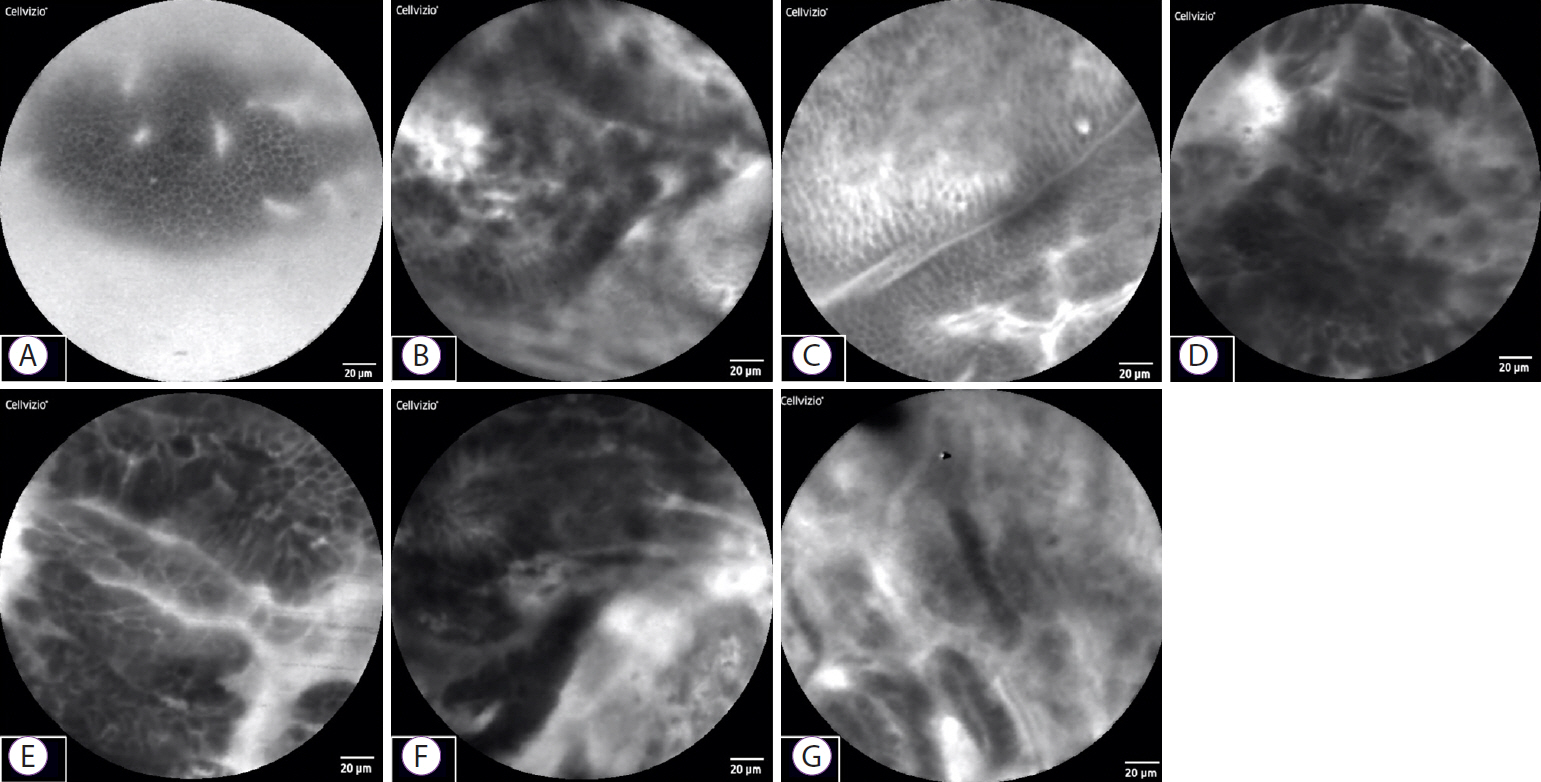
Fig. 4. Representative probe-based confocal laser endomicroscopy epithelial findings in 7 cases. (A) Cases 1 and 3: benign stricture due to surgery. Sheet-like monolayer of uniform epithelial cells. (B, D, E, F) Cases 2, 4, 5, and 6: bile duct cancer. Each cell is heterogeneous, and cells overlap and differ in size. (C) Case 3: normal bile duct. Sheet-like monolayer of uniform epithelial cells. (G) Case 7: IgG4-related sclerosing cholangitis. Cells are not sheet-like, but are relatively uniform in size, with no apparent overlap.
Reference
-
1. Ponchon T, Gagnon P, Berger F, et al. Value of endobiliary brush cytology and biopsies for the diagnosis of malignant bile duct stenosis: results of a prospective study. Gastrointest Endosc. 1995; 42:565–572.
Article2. Schoefl R, Haefner M, Wrba F, et al. Forceps biopsy and brush cytology during endoscopic retrograde cholangiopancreatography for the diagnosis of biliary stenoses. Scand J Gastroenterol. 1997; 32:363–368.
Article3. Rösch T, Hofrichter K, Frimberger E, et al. ERCP or EUS for tissue diagnosis of biliary strictures? A prospective comparative study. Gastrointest Endosc. 2004; 60:390–396.
Article4. Meining A, Chen YK, Pleskow D, et al. Direct visualization of indeterminate pancreaticobiliary strictures with probe-based confocal laser endomicroscopy: a multicenter experience. Gastrointest Endosc. 2011; 74:961–968.
Article5. Caillol F, Filoche B, Gaidhane M, Kahaleh M. Refined probe-based confocal laser endomicroscopy classification for biliary strictures: the Paris classification. Dig Dis Sci. 2013; 58:1784–1789.
Article6. Wallace M, Lauwers GY, Chen Y, et al. Miami classification for probe-based confocal laser endomicroscopy. Endoscopy. 2011; 43:882–891.
Article7. Kahaleh M, Giovannini M, Jamidar P, et al. Probe-based confocal laser endomicroscopy for indeterminate biliary strictures: refinement of the image interpretation classification. Gastroenterol Res Pract. 2015; 2015:675210.
Article8. Slivka A, Gan I, Jamidar P, et al. Validation of the diagnostic accuracy of probe-based confocal laser endomicroscopy for the characterization of indeterminate biliary strictures: results of a prospective multicenter international study. Gastrointest Endosc. 2015; 81:282–290.
Article9. Meining A, Shah RJ, Slivka A, et al. Classification of probe-based confocal laser endomicroscopy findings in pancreaticobiliary strictures. Endoscopy. 2012; 44:251–257.
Article10. Shieh FK, Drumm H, Nathanson MH, Jamidar PA. High-definition confocal endomicroscopy of the common bile duct. J Clin Gastroenterol. 2012; 46:401–406.
Article11. Blair NP, Evans MA, Lesar TS, Zeimer RC. Fluorescein and fluorescein glucuronide pharmacokinetics after intravenous injection. Invest Ophthalmol Vis Sci. 1986; 27:1107–1114.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Review of Probe-Based Confocal Laser Endomicroscopy for Pancreaticobiliary Disease
- Confocal Laser Endomicroscopy and Molecular Imaging in Barrett Esophagus and Stomach
- Probe-based confocal laser endomicroscopy in the differential diagnosis of inflammatory bowel diseases: a case series
- Usefulness of Probe-Based Confocal Laser Endomicroscopy for Esophageal Squamous Cell Neoplasm
- Confocal Laser Endomicroscopy in the Diagnosis of Biliary and Pancreatic Disorders: A Systematic Analysis
