Open Repair of Triangular Fibrocartilage Complex Type 1B Tear
- Affiliations
-
- 1Upper Extremity and Microsurgery Center, Department of Orthopedic Surgery, Semyeong Christianty Hospital, Pohang, Korea. osdrrih@gmail.com
- KMID: 2097614
- DOI: http://doi.org/10.12790/jkssh.2014.19.2.87
Abstract
- Most common traumatic type 1B tear of triangular fibrocartilage complex (TFCC), according to the Palmer's classification, may lead to the loss of the stability of distal radioulnar joint and is known to be one cause of the persisted ular side wrist pain. Recently as the knowledge of the anatomical structures of the TFCC accumulates and the deep fiber of the distal radioulnar ligament is recognized to play a central role, an attempt to repair it to the original ulnar fovea insertion site has been done and reported successful results. Since the introduction of open technique, numerous arthroscopic technique has been developing. Here careful considerations ought to be given during open repair will be taken with review of the related articles.
Figure
-

Fig. 1. (A-J) Pictures showing the operative procedure of the dorsal approach of open repair.
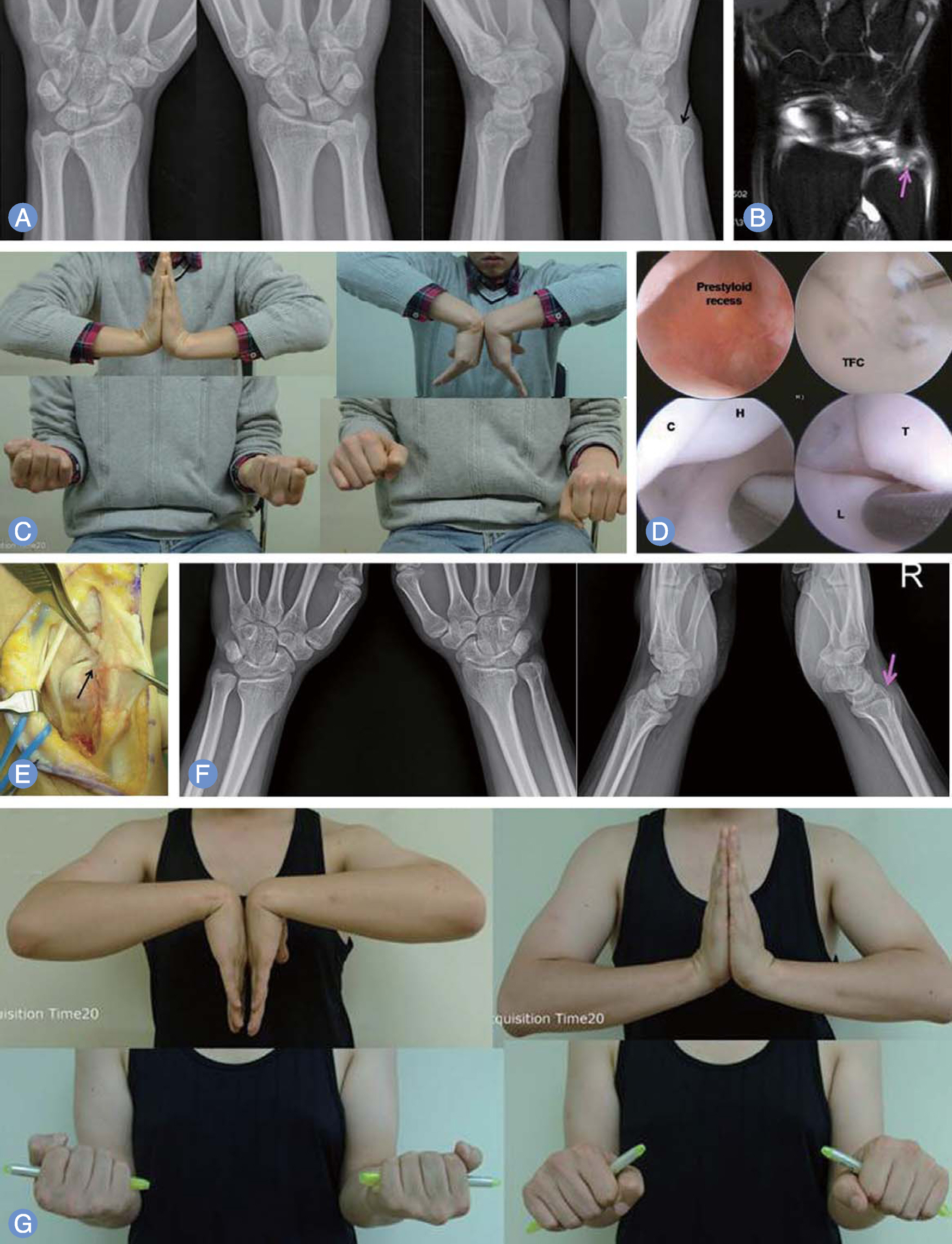
Fig. 2. Case of patient presenting with persisted ulnar side wrist pain after the initial injury 5 years ago. (A) Dorsal subluxation of the ulnar head (black arrow) on the lateral view of simple radiographs was found. (B) The detachment of deep fiber of triangular fibrocartilage complex (TFCC) from the ulnar fovea (pink arrow) was observed in coronal view of magnetic resonance imaging scans. (C) Slight restriction of the pronation was seen. (D) During the arthroscopic examination, synovitis around the prestyloid recess was found with the loss of the tension of the TFCC (positive trampoline test) and traction induced inward folding of the TFCC from the ulnar fovea (positive Hook test). Other combined injuries did not accompany. TFC, triangular fibrocartilage; C, capitate; H, hamate; L, lunate; T, triquetrum. (E) Open repair of the deep fiber of TFCC to the original ulnar fovea (black arrow) was done using the transosseous suture technique. (F) The reduced state of the preoperatively subluxated ulnar (pink arrow) head was seen on the follow-up radiographs taken at five years after operation. (G) Functional outcomes measured by Mayo modified wrist score and disability of the arm, shoulder and arm score improved from 55 preoperatively to 100 postoperatively and 35 to 3.3, separately.

Fig. 3. Case of patient presenting with persisted ulnar side wrist pain after the initial injury 6 months ago despite of the initial conservative management using long arm cast for 4 weeks. (A) Except the finding of the interpositional arthroplasty of fourth and fourth carpometacarpal joint of the right side (pink arrow), specific finding was not found around the ulnar head (pink circle). The detachment of deep fiber of triangular fibrocartilage complex (TFCC) from the ulnar fovea (pink arrow) was observed in coronal view of magnetic resonance imaging scans (B) and computed tomography arthrogam (black arrow) (C). (D) Slight restriction of the volar and dorsiflexion was seen preoperatively. (E) During the arthroscopic examination (black arrow), synovitis (black arrow) around the prestyloid recess was found with the loss of the tension of the TFCC (positive trampoline test) and traction induced inward folding of the TFCC from the ulnar fovea (positive Hook test). Other injuries of the capitohamate instability and lunotriquetral instability accompanied. TFC, triangular fibrocartilage; C, capitate; H, hamate; L, lunate; T, triquetrum. (F) Open repair of the deep fiber of TFCC to the original ulnar fovea was done using the transosseous suture technique. (G) On the intraoperative fluoroscopic examination, well-positioned screws at the lunotriqetral and capitohamate joints was observed with the temoporary fixation of the distal radioulnar joint using two 2.0 mm K-wires. (H) Solid union of the lunotriquetral and capitohamate joints was seen on the simple radiographs taken at seven months after operation. (G) Functional outcomes measured by Mayo modified wrist score and disability of the arm, shoulder and hand score improved from 55 preoperatively to 99 postoperatively and 28.3 to 15, separately. (I) Near full range of motion except the slight limitation of the volar flexion was recovered.
Reference
-
References
1. Stuart PR, Berger RA, Linscheid RL, An KN. The dorsopalmar stability of the distal radioulnar joint. J Hand Surg Am. 2000; 25:689–99.
Article2. Gofton WT, Gordon KD, Dunning CE, Johnson JA, King GJ. Soft-tissue stabilizers of the distal radioulnar joint: an in vitro kinematic study. J Hand Surg Am. 2004; 29:423–31.
Article3. Palmer AK. Triangular fibrocartilage disorders: injury patterns and treatment. Arthroscopy. 1990; 6:125–32.
Article4. Hagert E, Hagert CG. Understanding stability of the distal radioulnar joint through an understanding of its anatomy. Hand Clin. 2010; 26:459–66.
Article5. Estrella EP, Hung LK, Ho PC, Tse WL. Arthroscopic repair of triangular fibrocartilage complex tears. Arthroscopy. 2007; 23:729–37. 37 e1.
Article6. Hermansdorfer JD, Kleinman WB. Management of chronic peripheral tears of the triangular fibrocartilage complex. J Hand Surg Am. 1991; 16:340–6.
Article7. Cooney WP, Linscheid RL, Dobyns JH. Triangular fibrocartilage tears. J Hand Surg Am. 1994; 19:143–54.
Article8. Nakamura T, Sato K, Okazaki M, Toyama Y, Ikegami H. Repair of foveal detachment of the triangular fibrocartilage complex: open and arthroscopic transosseous techniques. Hand Clin. 2011; 27:281–90.
Article9. Garcia-Elias M, Smith DE, Llusa M. Surgical approach to the triangular fibrocartilage complex. Tech Hand Up Extrem Surg. 2003; 7:134–40.
Article10. Pederzini LA, Tosi M, Prandini M, Botticella C. All-inside suture technique for Palmer class 1B triangular fibrocartilage repair. Arthroscopy. 2007; 23:1130.e1–4.
Article11. Atzei A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur Vol. 2009; 34:582–91.
Article12. Bain GI, McGuire D, Lee YC, Eng K, Zumstein M. Anatomic foveal reconstruction of the triangular fibrocartilage complex with a tendon graft. Tech Hand Up Extrem Surg. 2014; 18:92–7.
Article13. Adams BD, Divelbiss BJ. Reconstruction of the post-traumatic unstable distal radioulnar joint. Orthop Clin North Am. 2001; 32:353–63.
Article14. Moritomo H. Advantages of open repair of a foveal tear of the triangular fibrocartilage complex via a palmar surgical approach. Tech Hand Up Extrem Surg. 2009; 13:176–81.
Article15. Moritomo H, Masatomi T, Murase T, Miyake J, Okada K, Yoshikawa H. Open repair of foveal avulsion of the triangular fibrocartilage complex and comparison by types of injury mechanism. J Hand Surg Am. 2010; 35:1955–63.
Article16. Anderson ML, Larson AN, Moran SL, Cooney WP, Amrami KK, Berger RA. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am. 2008; 33:675–82.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Knotless Repair
- Surgical Techniques for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Transosseous Repair
- The Short Term Results of All-inside Arthroscopic Repair of the Triangular Fibrocartilage Complex Type 1B Tear by Knotless Suture Anchor
- Current Treatment of Triangular Fibrocartilage Complex Injuries
- Clinical Outcomes of Open Surgical Repair for Triangular Fibrocartilage Complex Foveal Detachment
