Arthroscopic Repair for Traumatic Peripheral Tear of Triangular Fibrocartilage Complex
- Affiliations
-
- 1Department of Orthopedic Surgery, Sung Ae General Hospital, Seoul, Korea. chansaam@hanafos.com
- KMID: 2297514
- DOI: http://doi.org/10.12671/jkfs.2007.20.4.330
Abstract
- PURPOSE
To assess the results of an arthroscopic repair for traumatic peripheral tears of triangular fibrocartilage complex (TFCC, Palmer type Ib).
MATERIALS AND METHODS
10 patients with traumatic peripheral TFCC tear were treated with outside-in technique with arthroscope and evaluated with an average follow-up of 19 months (range, 15 to 28 months). The clinical outcomes were assessed with investigation of pain, range of motion, grip strength, return to job and patient's satisfaction.
RESULTS
The arthroscopic repair of traumatic peripheral TFCC tear resulted in significant pain relief and increase in functional ability of wrist, that is, 8 excellent, 1 good and 1 fair results. At last follow-up, the average of flexion was 79° (range 76~86°), average of extension was 78° (range 70~84°), average pronation was 85° (range 75~91°) and average supination was 87° (range 79~92°). Nine patients except one were back to their original job.
CONCLUSION
Arthroscopic repair of traumatic peripheral TFCC tear could be used for pain relief and increase in functional ability of wrist.
MeSH Terms
Figure
-

Fig. 1 Illustration of straight and curved spinal needles.
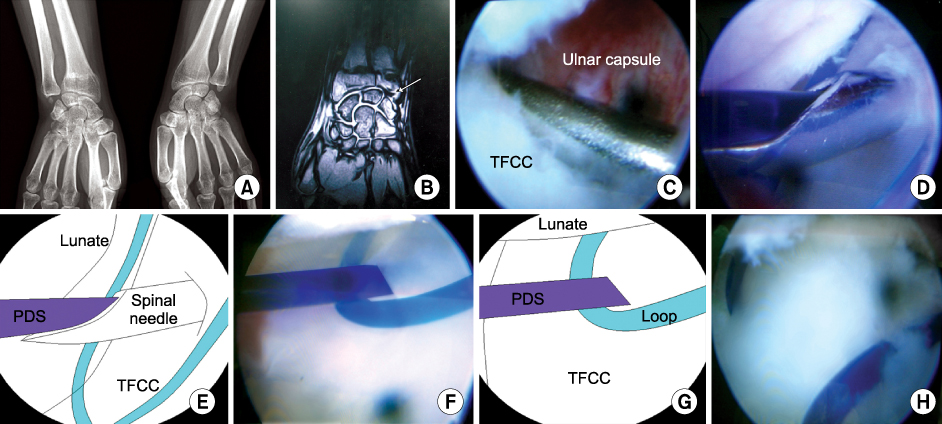
Fig. 2 This 33 year-old female patient suffered from right wrist pain due to slip down. (A) The wrist AP radiograph shows the old fracture of distal radius and non-union of ulnar styloid process. (B) T2 weighted coronal MR image shows the peripheral tear of TFCC (arrow). (C) Palmer type 1b TFCC tear was obvious on the arthroscopic field after shaving the hypertrophied synovium. (D) Outside-in technique. The curved spinal needle was inserted through the ulnar capsule and triangular fibrocartilage. Then 2-0 PDS was inserted through this spinal needle. (E) Schematic drawing of Fig. 2D. (F) 2-0 PDS was remained inside the loop which was inserted into the joint cavity through the straight spinal needle. (G) Schematic drawing of Fig. 2F. (H) The triangular fibrocartilage was tied to the capsule of ulnar side.
Reference
-
1. Bednar MS, Arnoczky SP, Weiland AJ. The microvasculature of the triangular fibrocartilage complex: its clinical significance. J Hand Surg Am. 1991; 16:1101–1105.
Article2. Cooney WP, Linscheid RL, Dobyns JH. Triangular fibrocartilage tears. J Hand Surg Am. 1994; 19:143–154.
Article3. Corso SJ, Savoie FH, Geissler WB, Whipple TL, Jiminez W, Jenkins N. Arthroscopic repair of peripheral avulsions of the triangular fibrocartilage complex of the wrist. A multicenter study. Arthroscopy. 1997; 13:78–84.
Article4. Haugstvedt JR, Husby T. Results of repair of peripheral tears in the triangular fibrocartilage complex using an arthroscopic suture technique. Scand J Plast Reconstr Surg Hand Surg. 1999; 33:439–447.
Article5. Lee SB, Lee CB. Intraarticular soft tissue injuries in fractures of the distal radius. J Korean Soc Fract. 2001; 14:726–731.
Article6. Lee WY, Park BM, Lim DE, Song KS, Hong JW. Arthroscopically assisted fixation of intraarticular distal radial fractures. J Korean Soc Fract. 2003; 16:399–406.
Article7. Minami A, Ishikawa J, Suenaga N, Kasashima T. Clinical result of treatment of triangular fibrocartilage complex tear by arthroscopic debridement. J Hand Surg Am. 1996; 21:406–411.
Article8. Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg Am. 1989; 14:594–606.
Article9. Potter HG, Asnis-Ernberg L, Weiland AJ, Hotchkiss Rn, Peterson MG, McCormack RR Jr. The utility of high-resolution magnetic resonance imaging in the evaluation of the triangular fibrocartilage complex of the wrist. J Bone Joint Surg Am. 1997; 79:1675–1684.
Article10. Shionova K, Nakamura R, Imaeda T, Makino N. Arthrography is superior to magnetic resonance imaging for diagnosing injuries of the triangular fibrocartilage. J Hand Surg Br. 1998; 23:402–405.
Article11. Skie MC, Mekhail AO, Deitrich DR, Ebraheim NE. Operative technique for inside-out repair of the triangular fibrocartilage complex. J Hand Surg Am. 1997; 22:814–817.
Article12. Thiru RG, Ferlic DC, Clayton ML, McClure DC. Arterial anatomy of the triangular fibrocartilage of the wrist and its surgical significance. J Hand Surg Am. 1986; 11:258–263.
Article13. Trumble TE, Gibert M, Vedder N. Isolated tear of the triangular fibrocartilage. Management by early arthroscopic repair. J Hand Surg Am. 1997; 22:57–65.
Article14. Whipple TL. Arthroscopic surgery: the wrist. . Philadelphia, PA: JB Lippincott;1992. p. 103–118.15. Whipple TL, Marotta JJ, Powell JH 3rd. Technique of wrist arthroscopy. Arthroscopy. 1986; 2:244–252.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Knotless Repair
- Surgical Techniques for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Transosseous Repair
- Open Repair of Triangular Fibrocartilage Complex Type 1B Tear
- Arthroscopic Treatment for Triangular Fibrocartilage Complex Lesion
- Traumatic Triangular Fibrocartilage Complex Injuries and Instability of the Distal Radioulnar Joint
