Graft outflow vein unification venoplasty with superficial left hepatic vein branch in pediatric living donor liver transplantation using a left lateral section graft
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2505346
- DOI: http://doi.org/10.14701/ahbps.2020.24.3.326
Abstract
- Orifice size of the left hepatic vein trunk (LHV) in left lateral segment (LLS) grafts is often too small to perform direct anastomosis. A small superficial branch of LHV is encountered in approximately 30% of LLS grafts. Unification venoplasty of the LHV trunk and its superficial vein branch makes the orifice size of LLS outflow vein larger than the original size. We present refined surgical techniques for LHV unification venoplasty with a superficial LHV branch. The patient was a 5-month-old 9 kg-weighing girl with biliary atresia. Her general condition deteriorated, but there was low possibility of deceased donor liver allocation, thus living donor liver transplantation was performed using her mother’s LLS. The graft hepatic vein was widened through unification venoplasty of LHV and its superficial branch. Recipient hepatic vein orifice was widened through unification of three hepatic veins. The graft and recipient hepatic vein orifices were well matched in size, and they were anastomosed with 5-0 continuous sutures. The portal vein was reconstructed with interposition of cold-preserved external iliac vein homograft. The graft left hepatic artery was reconstructed using the recipient right hepatic artery and hepaticojejunostomy was performed. This patient recovered uneventfully and is doing well for 3 months to date. The unification venoplasty with LHV trunk and its superficial vein branch makes the size of LLS outflow vein definitely larger than the original size, thus it can be a useful technical option to reduce the risk of hepatic vein outflow obstruction in pediatric liver transplantation using a LLS graft.
Figure
-

Fig. 1 Intraoperative photographs of bench work. (A) A small superficial branch of the left hepatic vein is located at the left end of the left hepatic vein stump. (B and C) This vein branch was incised to expose the lumen. (D-F) A septum between the two vein orifices was incised and some intervening hepatic parenchyma was excised. (G and H) The two graft vein openings were unified with the use of continuous sutures using a 6-0 PDS.

Fig. 2 Intraoperative photographs of recipient hepatic vein preparation. (A) The native liver of the recipient was completely dissected. (B) The hepatic parenchyma was incised with a surgical knife. (C) A bulk of the hepatic parenchyma was left around the hepatic veins. (D) A longitudinal incision was applied at the hepatic parenchyma between the right and middle hepatic vein trunks, by which the attached parenchyma was separated. (E and F) The hepatic parenchyma was forcefully pulled out to detach from the hepatic vein stumps, and the septa between the right and middle hepatic veins and the middle and left hepatic veins were incised. (G and H) The defect at the anterior wall between the right and middle hepatic vein stumps was repaired with continuous sutures using a 6-0 PDS.

Fig. 3 Intraoperative photographs of recipient portal vein interposition with a cold-preserved external iliac vein homograft. (A) The recipient portal vein was dissected extensively to the porto-splenic vein junction. (B) The anterior wall of the portal vein was incised with deeply located clamping. (C-E) A vein homograft was anastomosed to the portal vein stump through a modified end-to-end method. (F) The interposed vein conduit was distended.

Fig. 4 Intraoperative photographs of graft hepatic vein reconstruction. (A) The right and left corners of the graft and recipient hepatic vein orifices were tagged with a 5-0 PDS. (B and C) Continuous sutures of the posterior wall continued from the left corner to the 6 o’clock direction. (D) Suturing continued toward the right corner after meticulous size patching. (E and F) Suturing continued to anastomose the anterior wall.

Fig. 5 Intraoperative photographs of graft portal vein reconstruction. (A and B) The interposed vein conduit was stretched toward the graft portal vein and the redundant portion was excised. (C) Portal vein anastomosis was performed with continuous sutures using a 6-0 PDS. (D) The reconstructed portal vein was distended after a graft reperfusion. The marked line at the conduit indicates the axial direction of 12 o’clock.
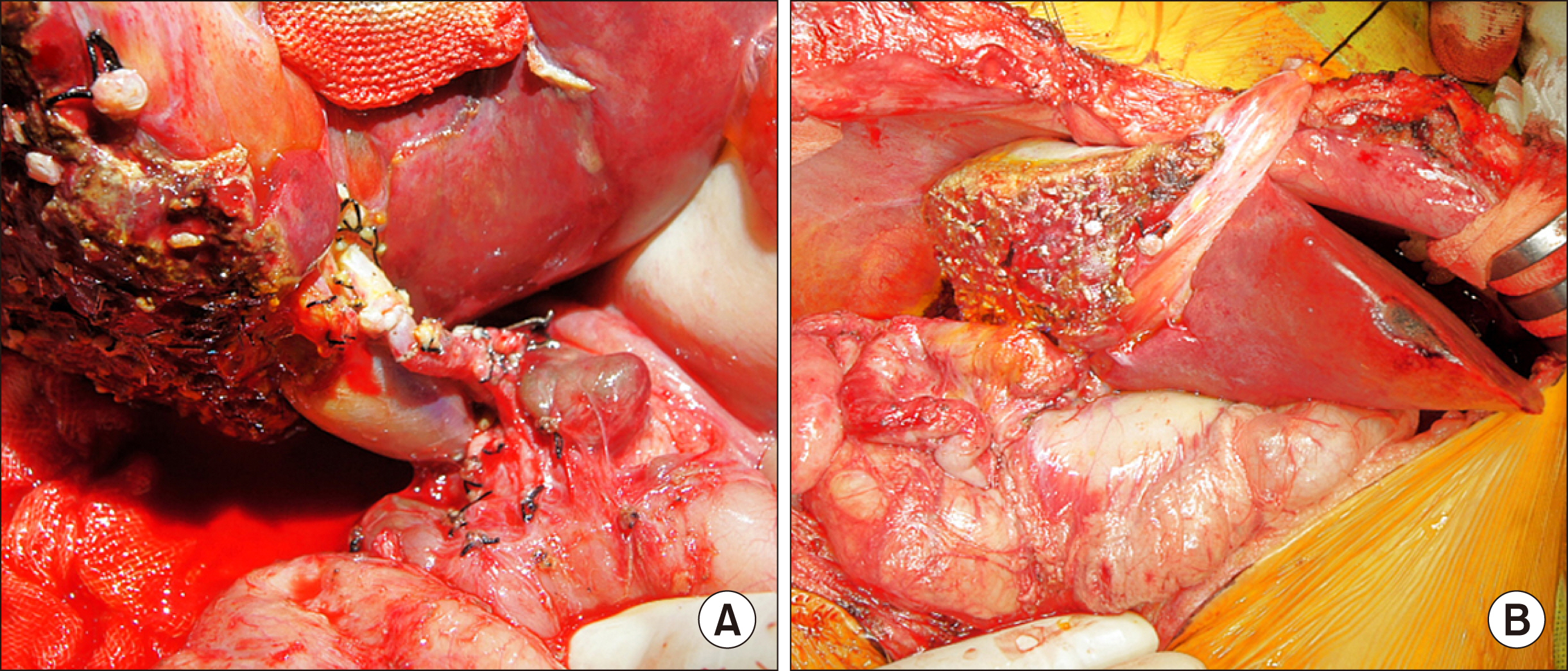
Fig. 6 Intraoperative photographs of reconstruction for graft hepatic artery and bile duct. (A) The graft left hepatic artery was reconstructed using the recipient right hepatic artery under surgical microscopy. (B) Hepaticojejunostomy was performed using the preformed Roux-en-Y jejunal limb.
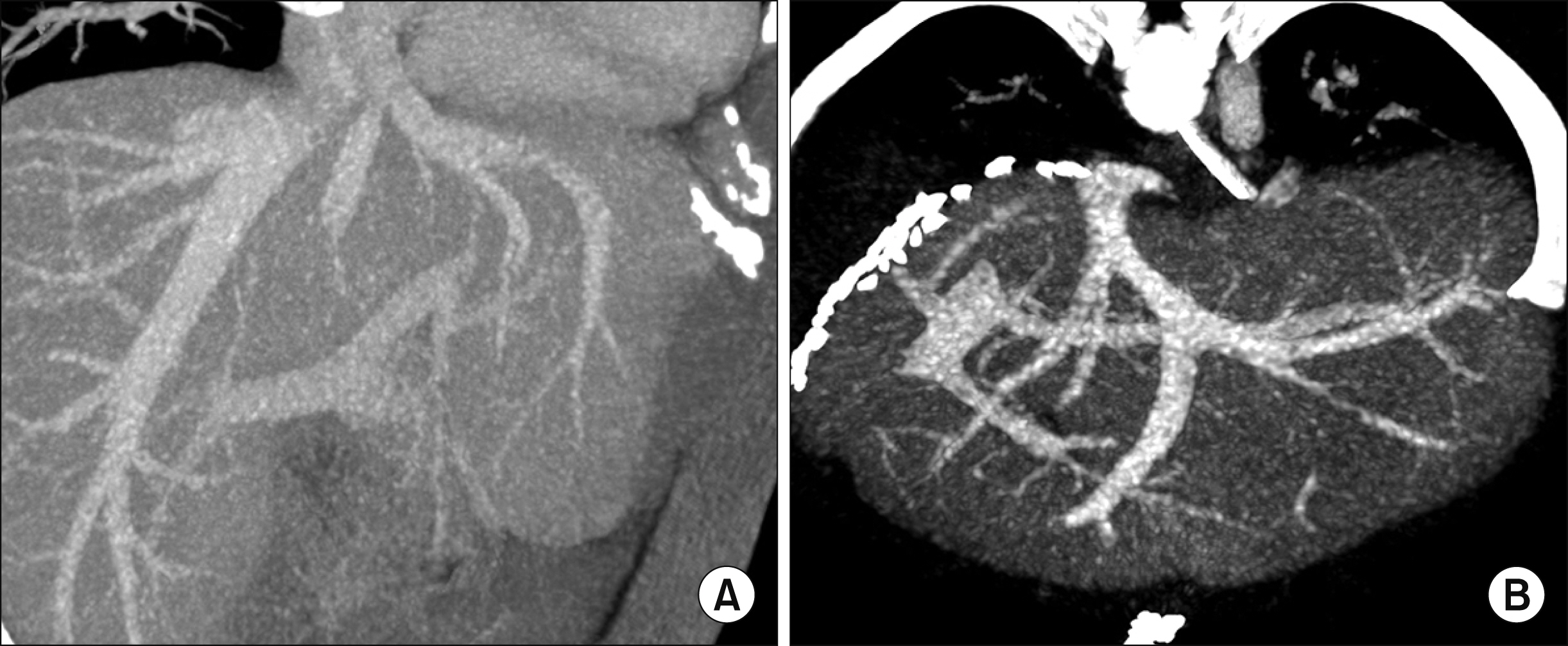
Fig. 7 Comparison of liver computed tomography (CT) scans before and after living donor liver transplantation. (A) Preoperative CT scan image shows the hepatic vein structures of the donor liver. (B) Recipient CT scan taken 5 days after transplantation shows the hepatic vein structures of the implanted left lateral section graft.
Cited by 3 articles
-
Pediatric liver transplantation with hyperreduced left lateral segment graft
Jung-Man Namgoong, Shin Hwang, Gi-Won Song, Dae-Yeon Kim, Tae-Yong Ha, Dong-Hwan Jung, Gil-Chun Park, Chul-Soo Ahn, Kyung Mo Kim, Seak Hee Oh, Hyunhee Kwon, Yong Jae Kwon
Ann Hepatobiliary Pancreat Surg. 2020;24(4):503-512. doi: 10.14701/ahbps.2020.24.4.503.Unification venoplasty of the outflow hepatic vein for laparoscopically harvested left liver grafts in pediatric living donor liver transplantation
Jung-Man Namgoong, Shin Hwang, Ki-Hun Kim, Gil-Chun Park, Kyung Mo Kim, Seak Hee Oh, Hwui-Dong Cho, Hyunhee Kwon, Yong Jae Kwon
Korean J Transplant. 2020;34(4):293-301. doi: 10.4285/kjt.20.0027.Third retransplantation using a whole liver graft for late graft failure from hepatic vein stent stenosis in a pediatric patient who underwent split liver retransplantation
Jung-Man Namgoong, Shin Hwang, Young-In Yoon, Yong-Pil Cho, Woo-Hyoung Kang, Yong Jae Kwon, Hyunhee Kwon, Sang Hoon Kim, Kyung Mo Kim, Seak Hee Oh
Ann Hepatobiliary Pancreat Surg. 2021;25(2):299-306. doi: 10.14701/ahbps.2021.25.2.299.
Reference
-
1. Karakayali H, Boyvat F, Coskun M, Isiklar I, Sözen H, Filik L, et al. 2006; Venous complications after orthotopic liver transplantation. Transplant Proc. 38:604–606. DOI: 10.1016/j.transproceed.2006.01.011. PMID: 16549187.
Article2. Hwang S, Lee SG, Choi ST, Moon DB, Ha TY, Lee YJ, et al. 2005; Hepatic vein anatomy of the medial segment for living donor liver transplantation using extended right lobe graft. Liver Transpl. 11:449–455. DOI: 10.1002/lt.20387. PMID: 15776411.
Article3. Hwang S, Kim DY, Ahn CS, Moon DB, Kim KM, Park GC, et al. 2013; Computational simulation-based vessel interposition reconstruction technique for portal vein hypoplasia in pediatric liver transplantation. Transplant Proc. 45:255–258. DOI: 10.1016/j.transproceed.2012.05.090. PMID: 23375311.
Article4. Galloux A, Pace E, Franchi-Abella S, Branchereau S, Gonzales E, Pariente D. 2018; Diagnosis, treatment and outcome of hepatic venous outflow obstruction in paediatric liver transplantation: 24-year experience at a single centre. Pediatr Radiol. 48:667–679. DOI: 10.1007/s00247-018-4079-y. PMID: 29468367.
Article5. Katano T, Sanada Y, Hirata Y, Yamada N, Okada N, Onishi Y, et al. 2019; Endovascular stent placement for venous complications following pediatric liver transplantation: outcomes and indications. Pediatr Surg Int. 35:1185–1195. DOI: 10.1007/s00383-019-04551-9. PMID: 31535198.
Article6. Zhang ZY, Jin L, Chen G, Su TH, Zhu ZJ, Sun LY, et al. 2017; Balloon dilatation for treatment of hepatic venous outflow obstruction following pediatric liver transplantation. World J Gastroenterol. 23:8227–8234. DOI: 10.3748/wjg.v23.i46.8227. PMID: 29290659. PMCID: PMC5739929.
Article7. Lu KT, Cheng YF, Chen TY, Tsang LC, Ou HY, Yu CY, et al. 2018; Efficiency of transluminal angioplasty of hepatic venous outflow obstruction in pediatric liver transplantation. Transplant Proc. 50:2715–2717. DOI: 10.1016/j.transproceed.2018.04.022. PMID: 30401383.
Article8. Yeh YT, Chen CY, Tseng HS, Wang HK, Tsai HL, Lin NC, et al. 2017; Enlarging vascular stents after pediatric liver transplantation. J Pediatr Surg. 52:1934–1939. DOI: 10.1016/j.jpedsurg.2017.08.060. PMID: 28927979.
Article9. Veerankutty FH, Ali TU, Manoj KS, Venugopal B. 2016; Reconstruction of a rare variant of the left hepatic vein in a left lateral segment liver graft from a living donor: technical notes. J Indian Assoc Pediatr Surg. 21:41–43. DOI: 10.4103/0971-9261.171938. PMID: 26862296. PMCID: PMC4721129.
Article10. Imamura H, Makuuchi M, Sakamoto Y, Sugawara Y, Sano K, Nakayama A, et al. 2000; Anatomical keys and pitfalls in living donor liver transplantation. J Hepatobiliary Pancreat Surg. 7:380–394. DOI: 10.1007/s005340070033. PMID: 11180859.
Article11. Matsunami H, Makuuchi M, Kawasaki S, Hashikura Y, Ikegami T, Nakazawa Y, et al. 1995; Venous reconstruction using three recipient hepatic veins in living related liver transplantation. Transplantation. 59:917–919. DOI: 10.1097/00007890-199503270-00024. PMID: 7701594.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Graft outflow vein venoplasty for a laparoscopically harvested left lateral section graft in pediatric living donor liver transplantation
- Outflow vein venoplasty of left lateral section graft for living donor liver transplantation in infant recipients
- Unification venoplasty of the outflow hepatic vein for laparoscopically harvested left liver grafts in pediatric living donor liver transplantation
- Incidence of superficial left hepatic vein and its usability for graft hepatic vein venoplasty in pediatric liver transplantation
- Standardized surgical techniques for adult living donor liver transplantation using a modified right lobe graft: a video presentation from bench to reperfusion
