Kosin Med J.
2020 Jun;35(1):38-46. 10.7180/kmj.2020.35.1.38.
Clinical Usefulness of Contrast-Enhanced Computed Tomography in Patients with Non-Obstructive Acute Pyleonephritis
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea
- 2Department of Radiology, Presbyterian Medical Center, Jeonju, Korea
- KMID: 2503727
- DOI: http://doi.org/10.7180/kmj.2020.35.1.38
Abstract
Objectives
The aim of this study is to investigate the clinical utility of contrast-enhanced computed tomography (CECT) in patient with non-obstrcutive acute pyelonephritis (APN).
Methods
From 2007 to 2013, 537 APN patients who underwent a CE-CT scan within 24 hours after hospital admission were enrolled. We divided these patients into greater (50% or greater involvment, n = 143) and lesser (less than 50% involvement, n = 394) groups based on renal parenchymal involvement in CE-CT examination. We compared clinical characteristics between two groups and analyzed the clinical value of CE-CT scan as a reliable marker for predicting clinical severity and disease course in patient with non-obstructive APN.
Results
The mean estimated glomerular filtration rate was 70.6 ± 25.5 mL/min/1.73m2. Compared with patients in lesser group, the patients in greater group had lower serum albumin levels (3.5 ± 0.5 vs 3.8 ± 0.6, P < 0.01) and longer hosptal stay (10.1 ± 4.7 vs 8.8 ± 4.5, P < 0.05). In addition, acute kidney injury (AKI) (23.1% vs 11.4%, P < 0.005) and bacteremia (36.4% vs 26.8%, P = 0.02) were frequently developed in greater group, respectively. The overall incidence of AKI was 14.8% based on RIFLE criteria. In a multivariate logistic regression analysis for predciting AKI, age, presence of diabetes mellitus and the presence of renal parenchymal involvement of greater than 50% in CE-CT were significant predictors of AKI.
Conclusions
The CE-CT scan could be useful to predict the clinical severity and course in non-obstructive APN patients with preserved renal function.
Figure
-
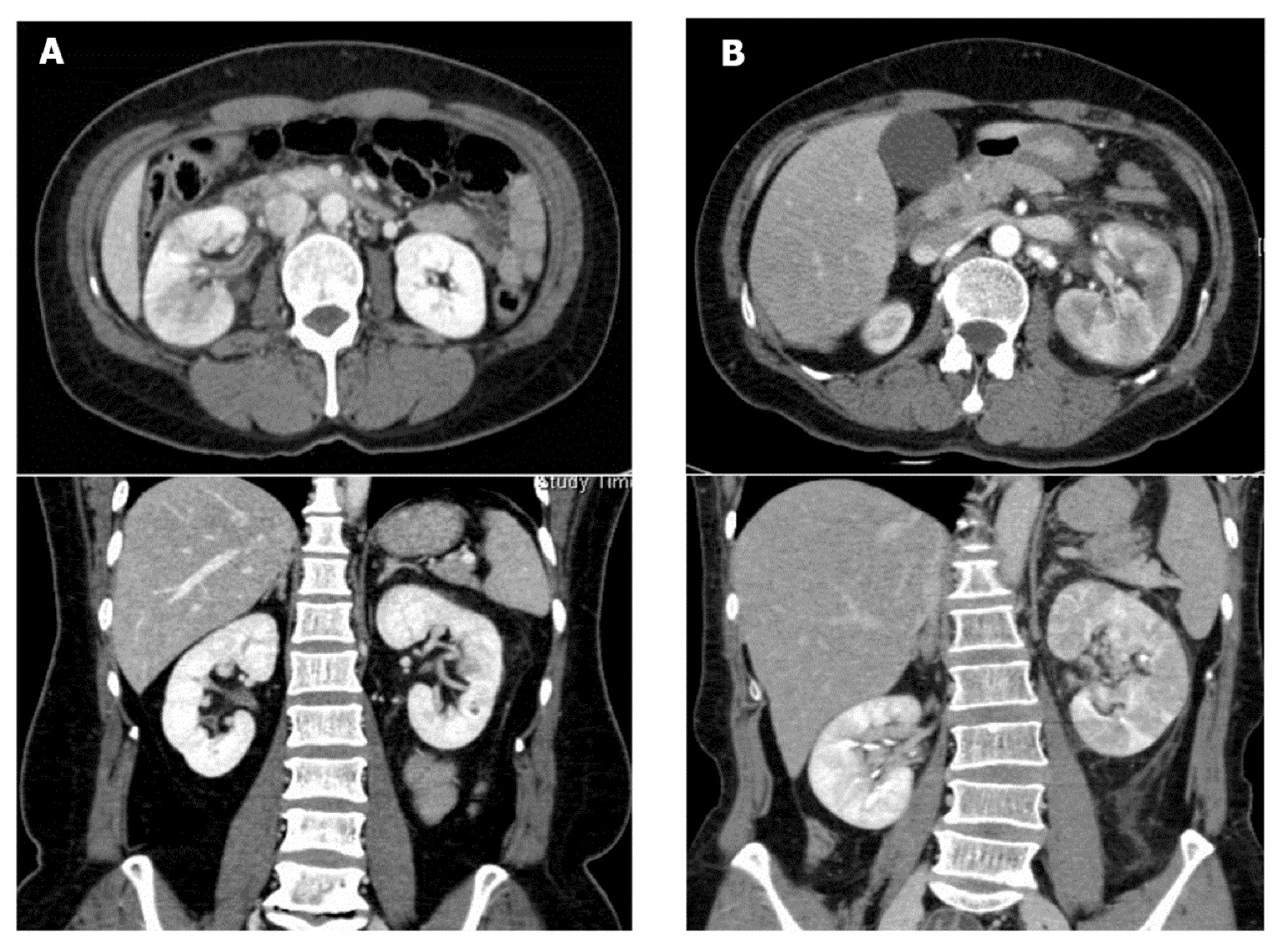
Fig. 1 Acute pyelonephritis grades according to CT findings. (A) lesser grade, lesser than 50% of renal involvement (B) greater grade, greater than 50% of renal involvement.
Reference
-
1. Bass PF 3d, Jarvis JA, Mitchell CK. Urinary tract infections. Prim Care. 2003; 30:41–61.
Article2. Nicolle LE. Urinary Tract infection. Crit Care Clin. 2013; 29:699–715.
Article3. Lee JH, Lee YM, Cho JH. Risk factors of septic shock in bacteremic acute pyelonephritis patients admitted to an ER. J Infect Chemother. 2012; 18:130–3.
Article4. Marschall J, Zhang L, Foxman B, Warren DK, Henderson JP. CDC Prevention Epicenters Program. Both host and pathogen factors predispose to Escherichia coli urinary-source bacteremia in hospitalized patients. Clin Infect Dis. 2012; 54:1692–8.
Article5. Rabushka LS, Fishman EK, Goldman SM. Pictorial review: computed tomography of renal inflammatory disease. Urology. 1994; 44:473–80.6. Kim JS, Lee S, Lee KW, Kim JM, Kim YH, Kim ME. Relationship between uncommon computed tomography findings and clinical aspects in patients with acute pyelonephritis. Korean J Urol. 2014; 55:482–6.
Article7. Soluen MC, Fisherman EK, Goldman SM, Gatewood OM. Bacterial renal infection: role of CT. Radiology. 1989; 171:703–7.
Article8. Gold RP, McClennan BL, Rottenberg RR. CT appearance of acute inflammatory disease of the renal interstitium. AJR Am J Roentgenol. 1983; 141:343–9.
Article9. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012; 120:c179–84.
Article10. Kim MH, Koh SO, Kim EJ, Cho JS, Na SW. Incidence and outcome of contrast-associated acute kidney injury assessed with Risk, Injury, Failure, Loss, and End-stage kidney disease (RIFLE) criteria in critically ill patients of medical and surgical intensive care units: a retrospective study. BMC Anesthesiol. 2015; 15:23.
Article11. Levey AS, Coresh J, Greene T, Marsh J, Stevens LA, Kusek JW, et al. Expressing the Modification of Diet in Renal Disease Study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem. 2007; 53:766–72.
Article12. Ki M, Park T, Choi B, Foxman B. The epidemiology of acute pyelonephritis in South Korea, 1997–1999. Am J Epidemiol. 2004; 160:985–93.
Article13. Leligdowicz A, Dodek PM, Norena M, Wong H, Kumar A, Kumar A, et al. Association between source of infection and hospital mortality in patients who have septic shock. Am J Respir Crit Care Med. 2014; 18(9):1204–13.
Article14. Paick SH, Choo GY, Baek M, Bae SR, Kim HG, Lho YS, et al. Clinical value of acute pyelonephritis grade based on computed tomography in predicting severity and course of acute pyelonephritis. J Comput Assist Tomogr. 2013; 37:440–2.
Article15. Yu TY, Kim HR, Hwang KE, Lee JM, Cho JH, Lee JH. Computed tomography findings associated with bacteremia in adult patients with a urinary tract infection. Eur J Clin Microbiol Infect Dis. 2016; 35:1883–7.
Article16. Oh SJ, Je BK, Lee SH, Choi WS, Hong D, Kim SB. Comparision of computed tomography findings between bacteremic and nonbacteremic acute pyelonephritis due to Escherichia coli. World J Radiol. 2016; 28(4):03–9.17. Lee H, Lee YS, Jeong R, Kim YJ, Ahn S. Predictive factors of bacteremia in patients with febrile urinary tract infection: an experience at a teritary care center. Infection. 2014; 42:669–74.18. Kim KS, Kim K, Jo YH, Kim TY, Lee JH, Lee SJ, et al. A simple model to predict bacteremia in women with acute pyelonephritis. J Infect. 2011; 63:124–30.
Article19. Macedo E, Mehta RL. Prerenal failure: from old concepts to new paradigms. Curr Opin Crit Care. 2009; 15:467–73.
Article20. Blantz RC, Singh P. Analysis of the Prerenal Contributions to Acute Kidney injury. Contrib Nephrol. 2011; 174:4–11.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Diagnostic Value of Contrast-Enhanced CT in Acute Bilateral Renal Cortical Necrosis: A Case Report
- Preparative fasting before contrast-enhanced computed tomography
- Massive Intraventricular Air Embolism after Contrast-enhanced CT: Report of Two Cases
- Decision Factors in Performance of Intravenous Contrast-enhanced Computed Tomography for Patients with Acute Flank Pain in an Emergency Department
- Comparison of Non-contrast-Enhanced Computed Tomography and Intravenous Pyelogram for Detection of Patients With Urinary Calculi
