Anterolateral Minimally Invasive Plate Osteosynthesis of Distal Tibial Fractures Using an Anterolateral Locking Plate
- Affiliations
-
- 1Department of Orthopedic Surgery, Daejeon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Daejeon, Korea
- KMID: 2502904
- DOI: http://doi.org/10.14193/jkfas.2020.24.1.19
Abstract
- Purpose
Anterolateral minimally invasive plate osteosynthesis (MIPO) was performed to treat patients with distal tibial fractures associated with open fractures or extensive soft tissue injuries, which is limited medial MIPO. The treatment results of the anterolateral MIPO technique were evaluated and analyzed.
Materials and Methods
Seventeen patients with distal tibial fractures associated with an open fracture or large bullae formation on the distal tibia medial side were treated with anterolateral MIPO using anterolateral locking plates. Within 24 hours of visiting the emergency room, external fixation was applied, and the medial side wound was managed. After damage control, the anterolateral locking plate was applied using an anterolateral MIPO technique. The union time, nonunion, or malunion were evaluated with regular postoperative radiographs. The ankle range of motion, operative time, blood loss, Iowa score, and wound complications were investigated.
Results
Radiological evidence of bony union was obtained in all cases. The mean time to union was 16.7 weeks (12∼25 weeks). The mean operation time was 44.0 minutes. Regarding the ankle range of motion, the mean dorsiflexion was 15°, and the mean plantarflexion was 35°. Satisfactory results were obtained in 15 out of 17 cases; five results were classified as excellent, four were good, and six were fair. The mean blood loss was 125.2 mL. Two complications were recorded.
Conclusion
In distal tibial fractures with severe medial soft tissue damage caused by high-energy trauma, the staged anterolateral MIPO technique using anterolateral locking plates is a useful alternative treatment to achieving optimal wound care, rapid union with biological fixation, and intra-articular reduction.
Keyword
Figure
-
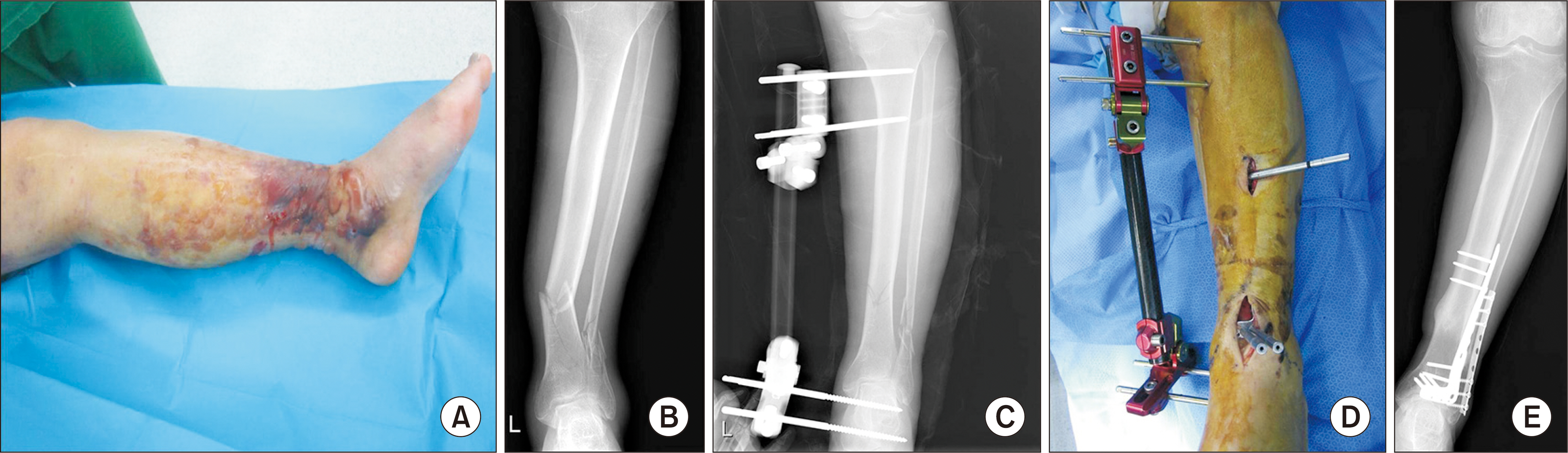
Figure 1. (A) A 71-year-old female was sustained distal tibia fracture with severe soft tissue swelling and blister. (B) Plain radiographs of the left ankle showed a distal tibial fracture of AO type A2 (AO Foundation/Orthopaedic Trauma Association classification). (C) A temporary external fixtor was applied to maintain for reduction of fracture, the length and alignment of the limb. (D) After the damage control, anterolateral plate was inserted through minimal anterior approach minimally invasive plate osteosynthesis (MIPO) technique. During anterolateral MIPO, an external fixator was used to maintain for reduction of the fracture. (E) At postoperative 1-year, the bony union of the fracture with callus site is visible.

Figure 2. (A) A 49-year-old female was sustained painful swelling and an open wound on the medial side of the right ankle due to a traffic accident. The fracture site of the distal tibia, which was a type IIIA open fracture, was exposed. (B) Plain radiographs of the left ankle showed a distal tibial fracture of AO type A1 (AO Foundation/Orthopaedic Trauma Association classification). (C) After the damage control by temporary external fixator, anterolateral plate was inserted through minimal anterior approach minimally invasive plate osteosynthesis (MIPO) technique. (D) Photograph after wound closure. Because anterolateral MIPO was performed, wound problems could be avoided. At postoperative 1-year, ankle anteroposterior (E) and lateral (F) plain radiographs show a bony union of the fracture site with callus formation.

Figure 3. The medial locking plate was exposed on medial side of the ankle.
Reference
-
References
1. Ahmad MA, Sivaraman A, Zia A, Rai A, Patel AD. Percutaneous locking plates for fractures of the distal tibia: our experience and a review of the literature. J Trauma Acute Care Surg. 2012; 72:E81–7. doi:. DOI: 10.1097/ta.0b013e3181f140b3.2. Borg T, Larsson S, Lindsjö U. Percutaneous plating of distal tibial fractures. Preliminary results in 21 patients. Injury. 2004; 35:608–14. doi:. DOI: 10.1016/j.injury.2003.08.015.3. Collinge C, Kuper M, Larson K, Protzman R. Minimally invasive plating of high-energy metaphyseal distal tibia fractures. J Orthop Trauma. 2007; 25:355–61. doi:. DOI: 10.1097/BOT.0b013e3180ca83c7.
Article4. Hasenboehler E, Rikli D, Babst R. Locking compression plate with minimally invasive plate osteosynthesis in diaphyseal and distal tibial fracture: a retrospective study of 32 patients. Injury. 2007; 38:365–70. doi:. DOI: 10.1016/j.injury.2006.10.024.
Article5. Helfet DL, Shonnard PY, Levine D, Borrelli J Jr. Minimally invasive plate osteosynthesis of distal fractures of the tibia. Injury. 1997; 28(Suppl 1):A42–7. ; discussion A47–8.
Article6. Helfet DL, Suk M. Minimally invasive percutaneous plate osteosynthesis of fractures of the distal tibia. Instr Course Lect. 2004; 53:471–5.7. Kim SK, Lee KB, Lim KY, Moon ES. Minimally invasive osteosynthesis with locking compression plate for distal tibia fractures. J Korean Fract Soc. 2011; 24:33–40. doi:. DOI: 10.12671/jkfs.2011.24.1.33.
Article8. Kim WY, Ji JH, Kwon OS, Park SE, Kim YY, Kil HJ, et al. Clinical features of distal tibial fractures and treatment results of minimally invasive plate osteosynthesis. J Korean Foot Ankle Soc. 2012; 16:94–100.9. Krackhardt T, Dilger J, Flesch I, Höntzsch D, Eingartner C, Weise K. Fractures of the distal tibia treated with closed reduction and minimally invasive plating. Arch Orthop Trauma Surg. 2005; 125:87–94. doi:. DOI: 10.1007/s00402-004-0778-y.
Article10. Lau TW, Leung F, Chan CF, Chow SP. Wound complication of minimally invasive plate osteosynthesis in distal tibia fractures. Int Orthop. 2008; 32:697–703. doi:. DOI: 10.1007/s00264-007-0384-z.
Article11. Lee KB. Distal tibia fracture: plate osteosynthesis. J Korean Fracture Soc. 2009; 22:306–313. doi:. DOI: 10.12671/jkfs.2009.22.4.306.
Article12. Oh CW, Kyung HS, Park IH, Kim PT, Ihn JC. Distal tibia metaphyseal fractures treated by percutaneous plate osteosynthesis. Clin Orthop Relat Res. 2003; 408:286-91.doi:. DOI: 10.1097/00003086-200303000-00038.
Article13. Yenna ZC, Bhadra AK, Ojike NI, ShahulHameed A, Burden RL, Voor MJ, et al. Anterolateral and medial locking plate stiffness in distal tibial fracture model. Foot Ankle Int. 2011; 32:630–7. doi:. DOI: 10.3113/FAI.2011.0630.
Article14. Park SK, Oh CW, Oh JK, Kim KH, Min WK, Park BC, et al. Staged minimally invasive plate osteosynthesis of distal tibial fractures. J Korean Fract Soc. 2010; 23:289–95. doi:. DOI: 10.12671/jkfs.2010.23.3.289.
Article15. Redfern DJ, Syed SU, Davies SJ. Fractures of the distal tibia: minimally invasive plate osteosynthesis. Injury. 2004; 35:615–20. doi:. DOI: 10.1016/j.injury.2003.09.005.
Article16. Ronga M, Shanmugam C, Longo UG, Oliva F, Maffulli N. Minimally invasive osteosynthesis of distal tibial fractures using locking plates. Orthop Clin North Am. 2009; 40:499–504. ix.doi:. DOI: 10.1016/j.ocl.2009.05.007.
Article17. Wyrsch B, McFerran MA, McAndrew M, Limbird TJ, Harper MC, Johnson KD, et al. Operative treatment of fractures of the tibial plafond. A randomized, prospective study. J Bone Joint Surg Am. 1996; 78:1646–57. doi:. DOI: 10.2106/00004623-199611000-00003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Percutaneous Plate Stabilization Using a Medial Locking Plate for Proximal Tibial Fractures: Technical Note
- Comparison of Results of Minimally Invasive Plate Osteosynthesis according to Types of Locking Plate in Distal Femoral Fractures
- Analysis of the Result Treated with Locking Compression Plate-Distal Tibia and Zimmer Periarticular Locking Plate in Distal Tibia Fracture
- Minimally Invasive Plate Osteosynthesis for Humeral Proximal or Distal Shaft Fractures Using a 3.5/5.0 Metaphyseal Locking Plate
- Clinical Outcomes of Locking Compression Plate Fixation through Minimally Invasive Percutaneous Plate Osteosynthesis in the Treatment of Distal Tibia Fracture
