Terminal Myelocystocele : Pathoembryogenesis and Clinical Features
- Affiliations
-
- 1Division of Pediatric Neurosurgery, Seoul National University Children's Hospital, Seoul, Korea
- 2Department of Anatomy and Cell Biology, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2501718
- DOI: http://doi.org/10.3340/jkns.2020.0063
Abstract
- There has been confusion in the classification of terminal myelocystocele (TMCC) due to its diverse morphology and vague pathoembryogenesis. TMCC could be summarized as having the essential features of an elongated caudal spinal cord extruding out of the dorsal extraspinal space that fuses with the subcutaneous fat, which is in the shape of a trumpet-shaped cerebrospinal fluid-filled cyst. The extraspinal portion of the extruded spinal cord is nonfunctional. The morphological features suggest that TMCC is formed during secondary neurulation, specifically the failure of the degeneration of the secondary neural tube near the time of the terminal balloon. This review discusses the definition, as well as the clinical and surgical features, of TMCC with special emphasis on its pathoembryogenesis.
Keyword
Figure
-
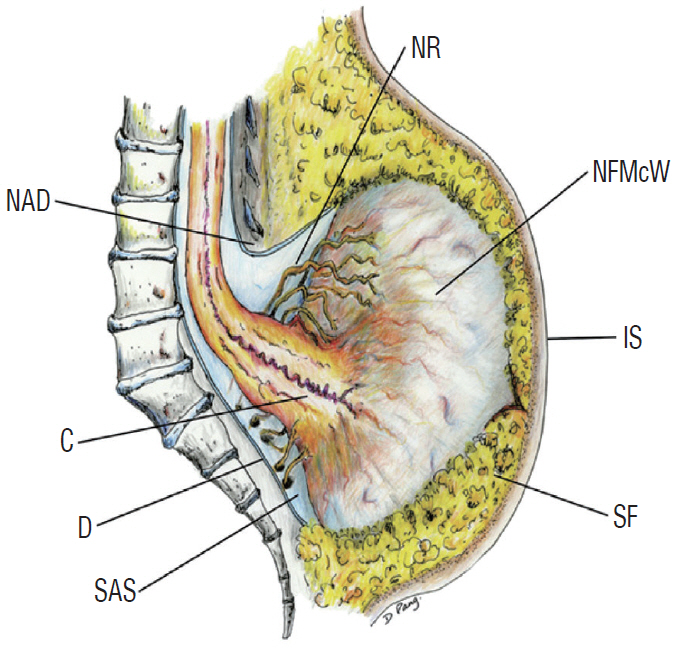
Fig. 1. A schematic drawing showing the essential features of terminal myelocystocele. The caudal end of the spinal cord is extended out of the spinal canal and attached to the subcutaneous fat in the shape of a flared trumpet. Adapted from Pang et al. [6] with permission from Oxford University Press. NR : functional sacral roots, NAD : neural arch defect, NFMcW : nonfunctional myelocystocele wall, C : conus, IS : intact skin, D : dura, SAS : subarachnoid space, SF : subcutaneous fat.
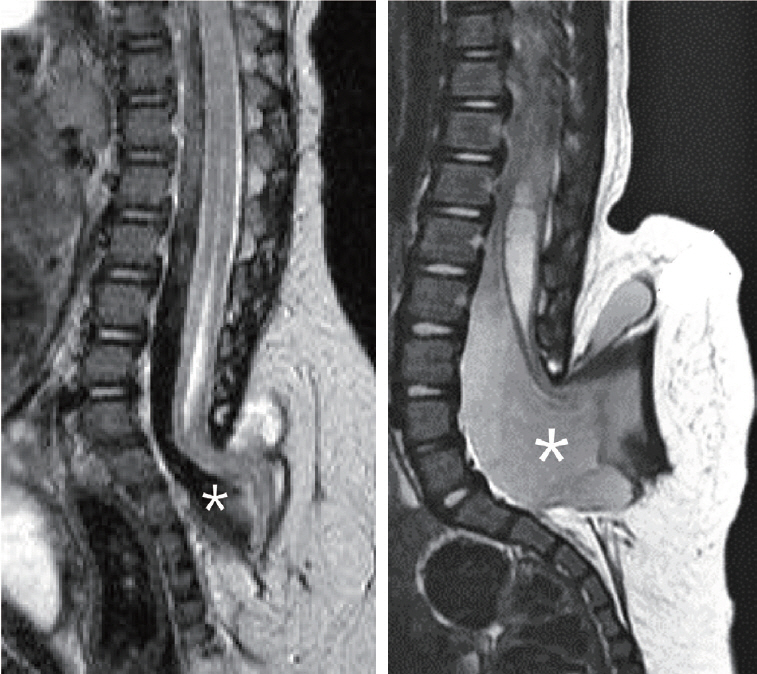
Fig. 2. Two cases of terminal myelocystocele showing a minimal amount of subarachnoid space (left) and a very wide extraspinal extension of the subarachnoid space (right). Asterisk (*) denotes the subarachnoid space in both pictures. Adapted from Pang et al. [6] with permission from Oxford University Press.
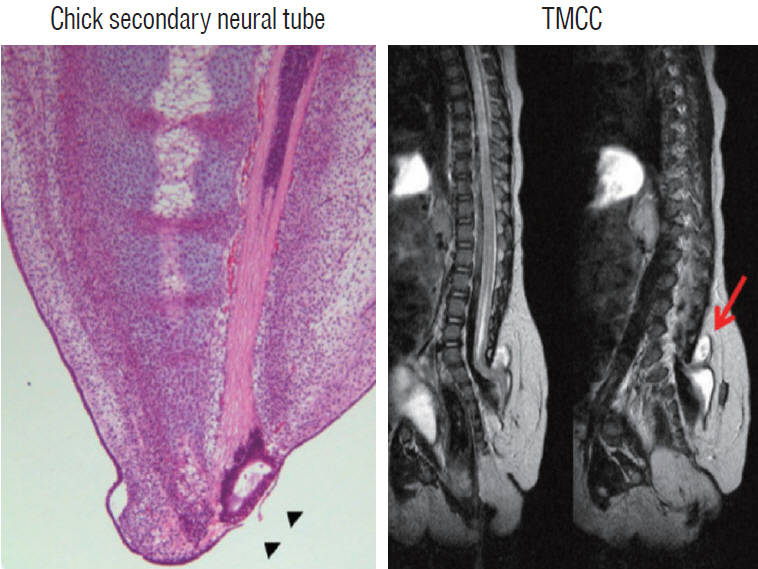
Fig. 3. The striking resemblance between chick secondary neurulation (left) and the sagittal MRI images of a prototypical TMCC patient (right). Note the apposition of the chick terminal balloon to the surface ectoderm (arrowheads), which is comparable to the subcutaneous position of the human TMCC (arrow). Adapted from Lee et al. [4] with permission from Springer Nature. MRI : magnetic resonance imaging, TMCC : terminal myelocystocele.
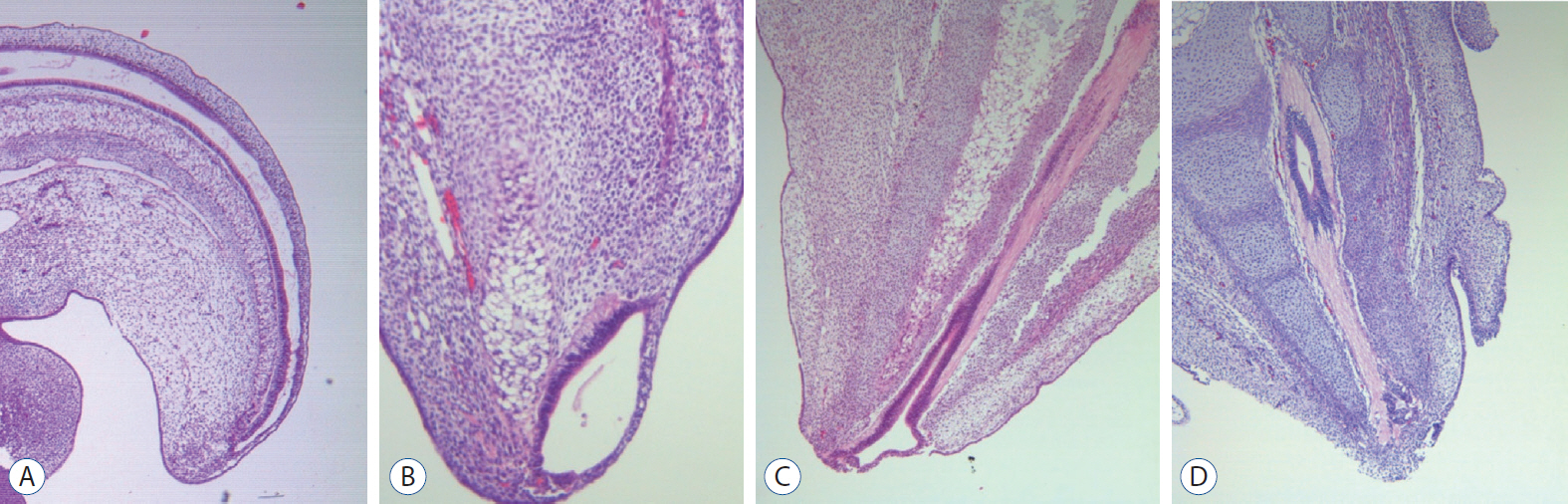
Fig. 4. A series of H&E images of the developing chick embryos showing the formation and degeneration of the terminal balloon. A : Formation of the cavitary conjoining of primary and secondary neural tubes (×40). B : Appearance of the terminal balloon (×100). C : Shrinkage of the terminal balloon (×40). D : Degeneration of the terminal balloon and detachment of the medullary cord from the surface ectoderm (×40).
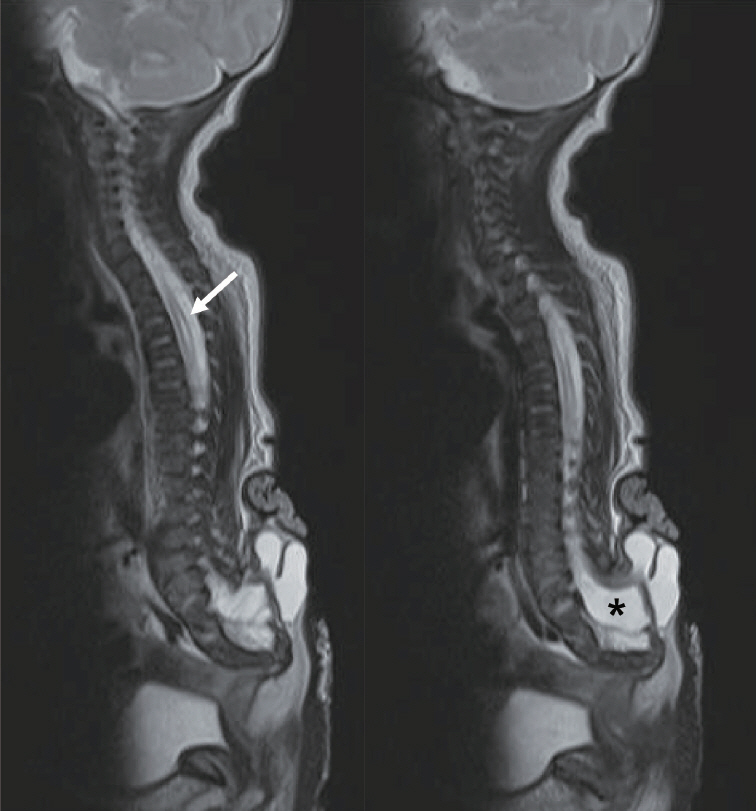
Fig. 5. A series of MRI T2 sagittal images of a 1-week-old girl with terminal myelocystocele. Note the extensively wide subarachnoid space (right, asterisk) and syringomyelia up to the upper thoracic level (left, arrow). MRI : magnetic resonance imaging.
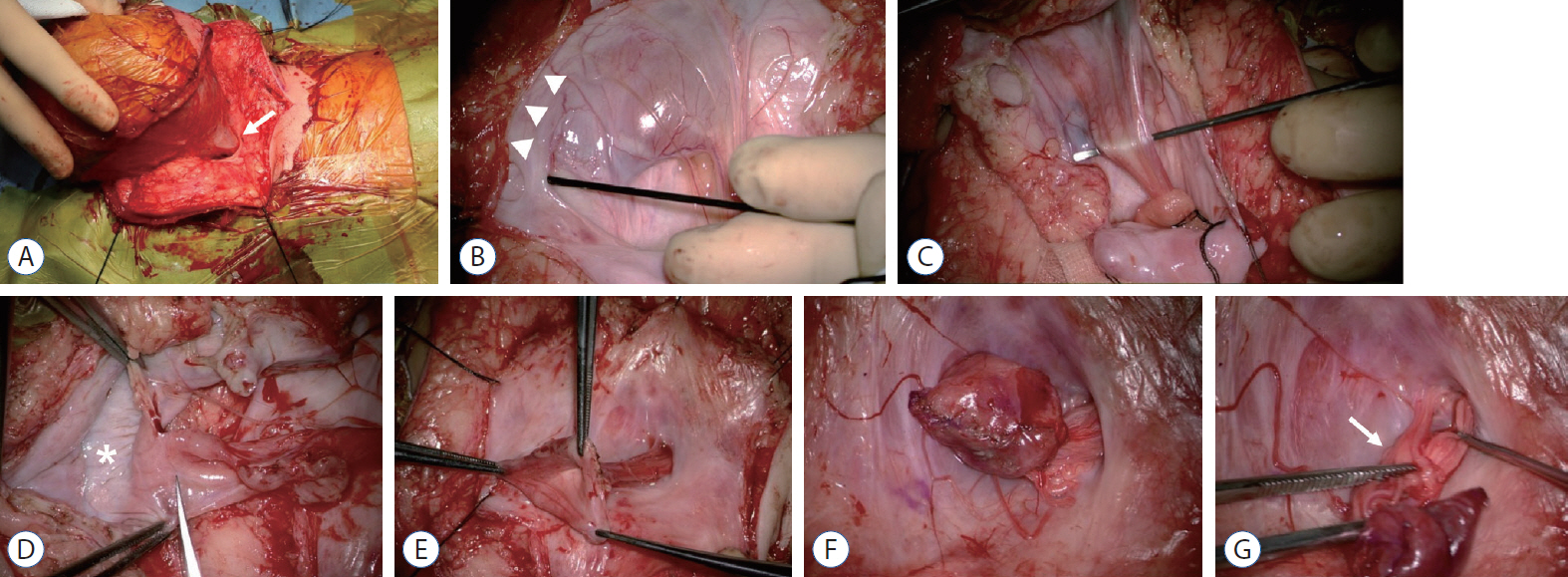
Fig. 6. Surgical sequence in a case with terminal myelocytocele. A : The neck of the trumpet (arrow) is seen extending out of the fascia defect into the huge sac. B : After dural opening, the margin at which the myelocystocele sac joins the subcutaneous fat is shown (arrowheads). C : The rostral spinal cord flares out into the proximal part of the enormous cyst. D : The sac wall is opened to expose the inner lining (asterisk), and a trimming of the margin of the neural placode is performed. Neural placode before (E) and after pial reconstruction (F). G : Nerve roots (arrow) arise from the basal side of the proximal sac and stream back into the spinal canal.
Reference
-
References
1. Barkovich AJ, Kuzniecky RI, Dobyns WB. Radiologic classification of malformations of cortical development. Curr Opin Neurol. 14:145–149. 2001.
Article2. Byrd SE, Harvey C, McLone DG, Darling CF. Imaging of terminal myelocystoceles. J Natl Med Assoc. 88:510–516. 1996.3. Choi S, McComb JG. Long-term outcome of terminal myelocystocele patients. Pediatr Neurosurg. 32:86–91. 2000.
Article4. Lee JY, Phi JH, Kim SK, Cho BK, Wang KC. Urgent surgery is needed when cyst enlarges in terminal myelocystoceles. Childs Nerv Syst. 27:2149–2153. 2011.
Article5. McLone DG, Naidich TP. Terminal myelocystocele. Neurosurgery. 16:36–43. 1985.
Article6. Pang D, Zovickian J, Lee JY, Moes GS, Wang KC. Terminal myelocystocele: surgical observations and theory of embryogenesis. Neurosurgery. 70:1383–1404. discussion 1404-1405. 2012.7. Tandon V, Garg K, Mahapatra AK. Terminal myelocystocele: a series of 30 cases and review of the literature. Pediatr Neurosurg. 48:229–235. 2012.
Article8. Yang HJ, Lee DH, Lee YJ, Chi JG, Lee JY, Phi JH, et al. Secondary neurulation of human embryos: morphological changes and the expression of neuronal antigens. Childs Nerv Syst. 30:73–82. 2014.
Article9. Yang HJ, Wang KC, Chi JG, Lee MS, Lee YJ, Kim SK, et al. Neural differentiation of caudal cell mass (secondary neurulation) in chick embryos: Hamburger and Hamilton Stages 16-45. Brain Res Dev Brain Res. 142:31–36. 2003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Terminal myelocystocele: a case report
- Terminal Myelocystocele: A Skin-Covered Lumbosacral Cystic Mass
- Disorders of Secondary Neurulation : Mainly Focused on Pathoembryogenesis
- Enlargement of Extraspinal Cysts in Spinal Dysraphism : A Reason for Early Untethering
- The Impact of Clinical Nurses' Terminal Care Attitude and Spiritual Health on Their Terminal Care Stress
