Enlargement of Extraspinal Cysts in Spinal Dysraphism : A Reason for Early Untethering
- Affiliations
-
- 1Division of Pediatric Neurosurgery, Seoul National University Children's Hospital, Seoul, Korea
- 2Department of Anatomy and Cell Biology, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2501721
- DOI: http://doi.org/10.3340/jkns.2020.0094
Abstract
- Some types of spinal dysraphism can be accompanied by extraspinal cysts, including myelomeningocele, myelocystocele, myelocele, meningocele, limited dorsal myeloschisis, lipomyelomeningocele, and terminal myelocystocele. Each disease is classified according to the developmental mechanism, embryologic process, site of occurrence, or internal structure of the extraspinal cyst. In most cystic spinal dysraphisms except meningocele, part of the spinal cord is attached to the cyst dome. Most open spinal dysraphisms pose a risk of infection and require urgent surgical intervention, but when the cyst is accompanied by closed spinal dysraphism, the timing of surgery may vary. However, if the extraspinal cyst grows, it aggravates tethering by pulling the tip of the cord, which is attached to the dome of the cyst. This causes neurological deficits, so urgent surgery is required to release the tethered cord.
Keyword
Figure
-
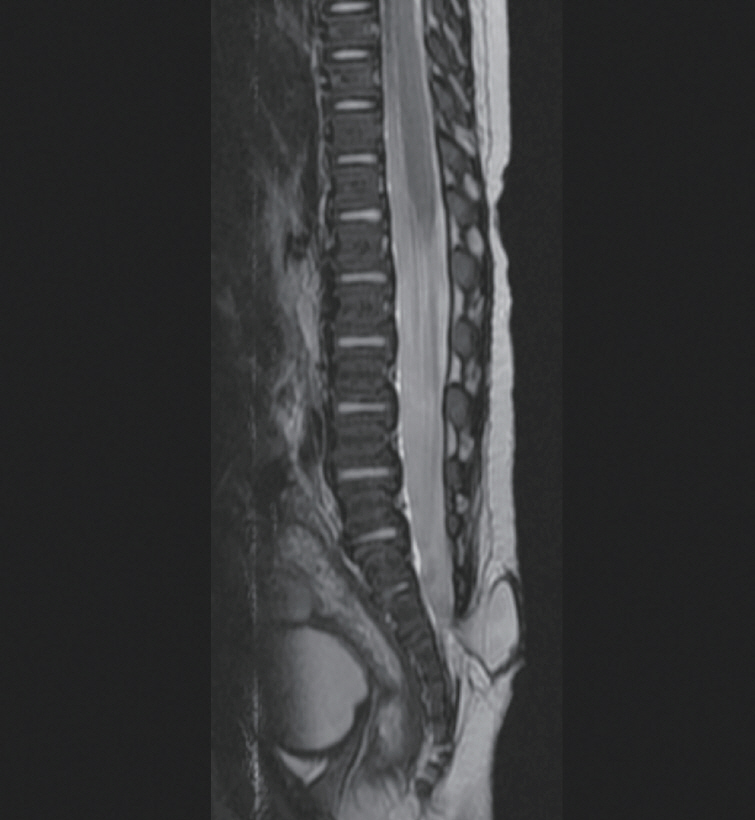
Fig. 1. Meningocele without any neural structure inside the sac.
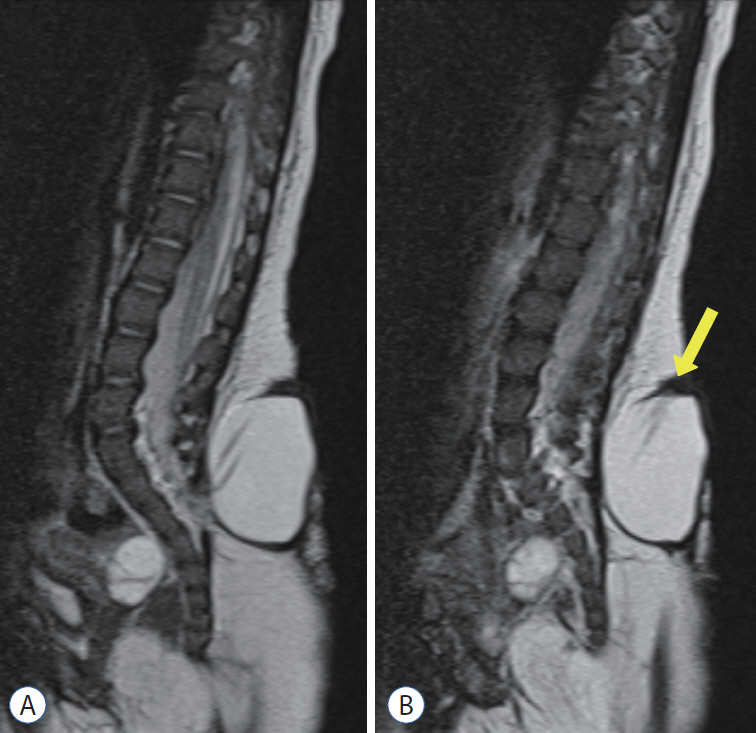
Fig. 2. A : Saccular type of limited dorsal myeloschisis. B : Note the stalk to dome (yellow arrow).
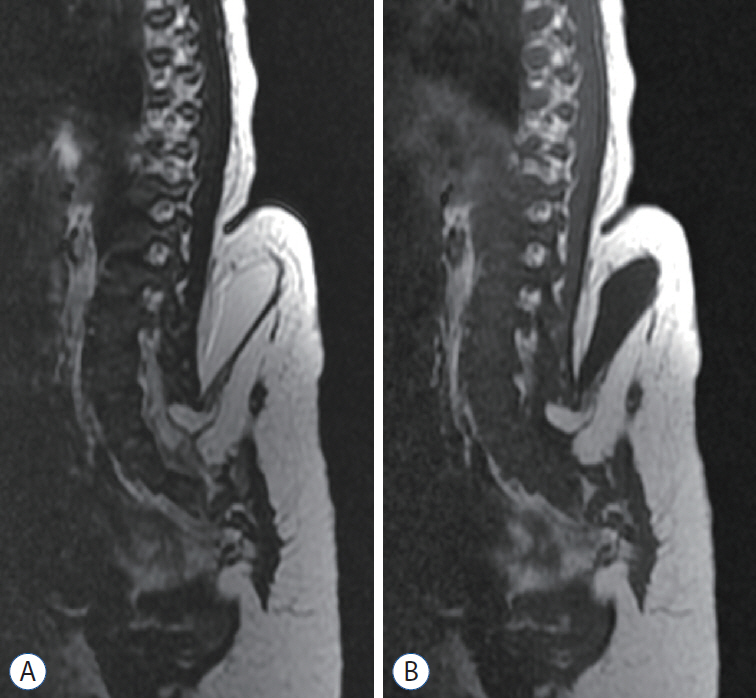
Fig. 3. ‘True’ lipomyelomeningocele shows the herniated spinal cord with fat tissue and cerebrospinal fluid in the dural sac through the fascial defect. A : T2-weighted imaging. B : T1-weighted imaging.
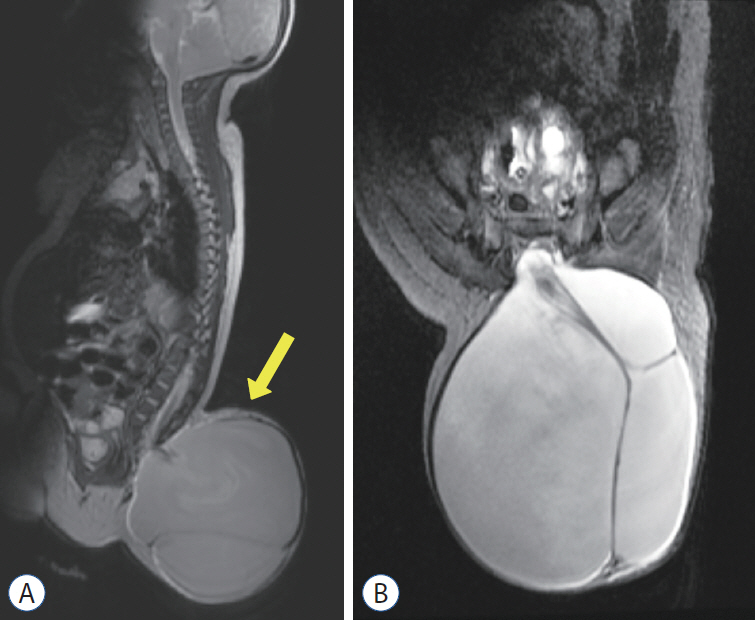
Fig. 4. Terminal myelocystocele. Note the low-lying syringomyelic spinal cord (yellow arrow). A : Sagittal section. B : Axial section.
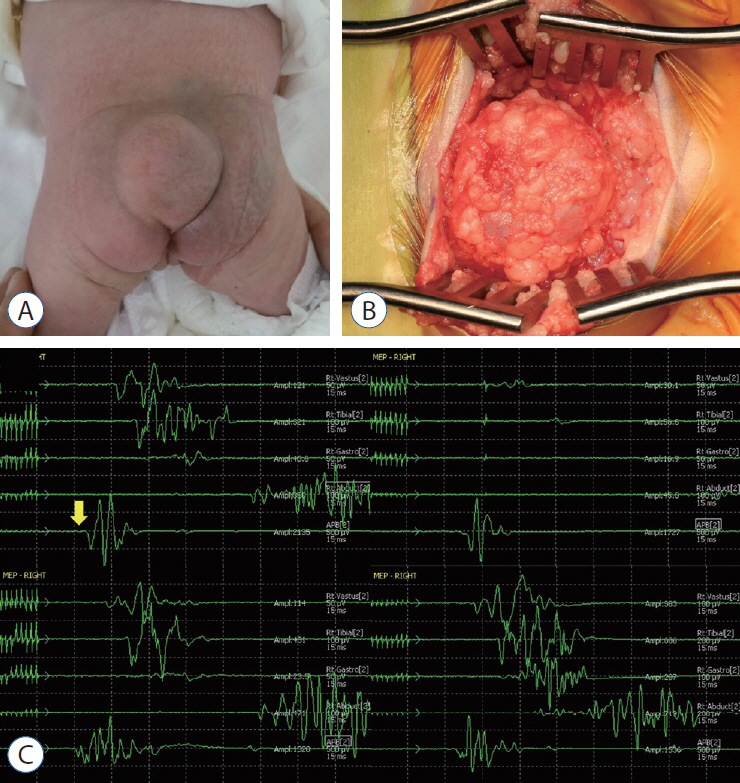
Fig. 5. A : A gross photo of the patient shows a cystic mass in the back. B : An operative photo shows the cystic mass herniated through the fascial defect (right - cephalad side of the patient). C : Tracings of motor evoked potentials (MEPs) demonstrate changes in MEPs during the operation. The baseline MEPs were recorded at the start of surgery (left upper). Decreases in MEPs in both lower extremities were noticed. Only the right-side tracings are shown in this figure (from top to bottom : vastus medialis, anterior tibialis, gastrocnemius, abductor hallucis, adductor pollicis brevis). Please note that there was no change in the control MEPs in the upper extremity from abductor pollicis brevis (yellow arrow) (right upper). After aspiration of cerebrospinal fluid, the signal appeared again immediately (left lower) and was fully recovered after 20 minutes (right lower). Adopted from Kim et al. [2], with permission from Springer Nature.
Cited by 1 articles
-
Disorders of Secondary Neurulation : Mainly Focused on Pathoembryogenesis
Jeyul Yang, Ji Yeoun Lee, Kyung Hyun Kim, Kyu-Chang Wang
J Korean Neurosurg Soc. 2021;64(3):386-405. doi: 10.3340/jkns.2021.0023.
Reference
-
References
1. Gupta DK, Mahapatra AK. Terminal myelocystoceles: a series of 17 cases. J Neurosurg. 103(4 Suppl):344–352. 2005.
Article2. Kim KH, Chong S, Lee JY, Kim K, Kim SK, Wang KC. Decreased MEPs during subcutaneous dissection for untethering surgery of a "true" lipomyelomeningocele: aggravated traction of the spinal cord by release of the sac from the original nest. Childs Nerv Syst. 35:529–533. 2019.
Article3. Kumar R, Chandra A. Terminal myelocystocele. Indian J Pediatr. 69:1083–1086. 2002.
Article4. Lee JY, Phi JH, Kim SK, Cho BK, Wang KC. Urgent surgery is needed when cyst enlarges in terminal myelocystoceles. Childs Nerv Syst. 27:2149–2153. 2011.
Article5. McLone DG, Naidich TP. Terminal Myelocystocele. Neurosurgery. 16:36–43. 1985.
Article6. Morioka T, Hashiguchi K, Yoshida F, Matsumoto K, Miyagi Y, Nagata S, et al. Neurosurgical management of occult spinal dysraphism associated with OEIS complex. Childs Nerv Syst. 24:723–729. 2008.
Article7. Pang D, Zovickian J, Lee JY, Moes GS, Wang KC. Terminal myelocystocele: surgical observations and theory of embryogenesis. Neurosurgery. 70:1383–1405. discussion 1404-1405. 2012.8. Wataya T, Horikawa K, Kitagawa M, Tashiro Y. Thoracic meningocele in lumbo-costo-vertebral syndrome in a child: possible enlargement with repeated motion by anchoring to the diaphragm. J Neurosurg Pediatr. 18:183–186. 2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Neurophysiology Monitoring for Spinal Dysraphism
- Intramedullary Spinal Cord Lipoma without Spinal Dysraphism
- Spinal Dysraphism and Tethered Cord Syndrome
- Multiple Lumbar Intradural Dermoid Cysts without Spinal Dysraphism
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
