Accuracy Analysis of Iliac Screw Using Freehand Technique in Spinal Surgery : Relation between Screw Breach and Revision Surgery
- Affiliations
-
- 1Department of Neurological Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Emergency Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
- 3Division of Orthopaedic Surgery, University Health Network, Toronto Western Hospital, Toronto, Canada
- KMID: 2501707
- DOI: http://doi.org/10.3340/jkns.2019.0090
Abstract
Objective
: To analyze the accuracy of iliac screws using freehand technique performed by the same surgeon. We also analyzed how the breach of iliac screws was related to the clinical symptoms resulting in revision surgery.
Methods
: From January 2009 to November 2015, 100 patients (193 iliac screws) were analyzed using postoperative computed tomography scans. The breaches were classified based on the superior, inferior, lateral, and medial iliac wall violation by the screw. According to the length of screw extrusion, the classification grades were as follows : grade 1, screw extrusion <1 cm; grade II, 1 cm ≤ screw extrusion <2 cm; grade III, 2 cm ≤ screw extrusion <3 cm; and grade IV, 3 cm ≤ screw extrusion. We also reviewed the revision surgery associated with iliac screw misplacement.
Results
: Of the 193 inserted screws, 169 were correctly located and 24 were misplaced screws. There were eight grade I, six grade II, six grade III, and four grade IV screw breaches, and 11, 8, 2, and 3 screws violated the medial, lateral, superior, and inferior walls, respectively. Four revision surgeries were performed for the grade III or IV iliac screw breaches in the lateral or inferior direction with respect to its related symptoms.
Conclusion
: In iliac screw placement, 12.4% breaches developed. Although most breaches were not problematic, symptomatic violations (2.1%) could result in revision surgery. Notably, the surgeon should keep in mind that lateral or inferior wall breaches longer than 2 cm can be risky and should be avoided.
Keyword
Figure
-
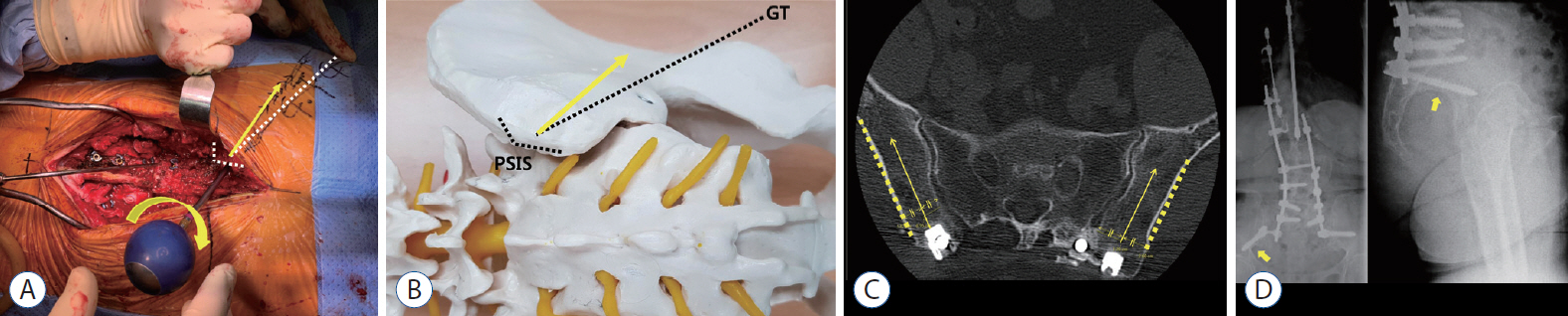
Fig. 1. A : Intraoperative photograph showing a screw trajectory with a pedicle probe after removal of the PSIS. First, the GT is palpated to identify it (white dotted line) and then it is used as a marker to advance the pedicle probe 15° above (yellow arrows). B : A model showing the screw entry point (center of the PSIS) and inferior angle (15° above the GT, yellow arrow). C : Postoperative computed tomography image showing that the screw entry point is located in the center of the PSIS (yellow arrows) and the pelvic lateral wall slope used for creating a lateral angle of the screw trajectory (yellow dotted lines). D : After screw insertion, portable anterior-posterior (AP) and lateral radiographs were obtained before the closure. In these images, the screw location was considered acceptable if it was above the sciatic notch (yellow arrows). PSIS : posterior superior iliac spine, GT : greater trochanter.
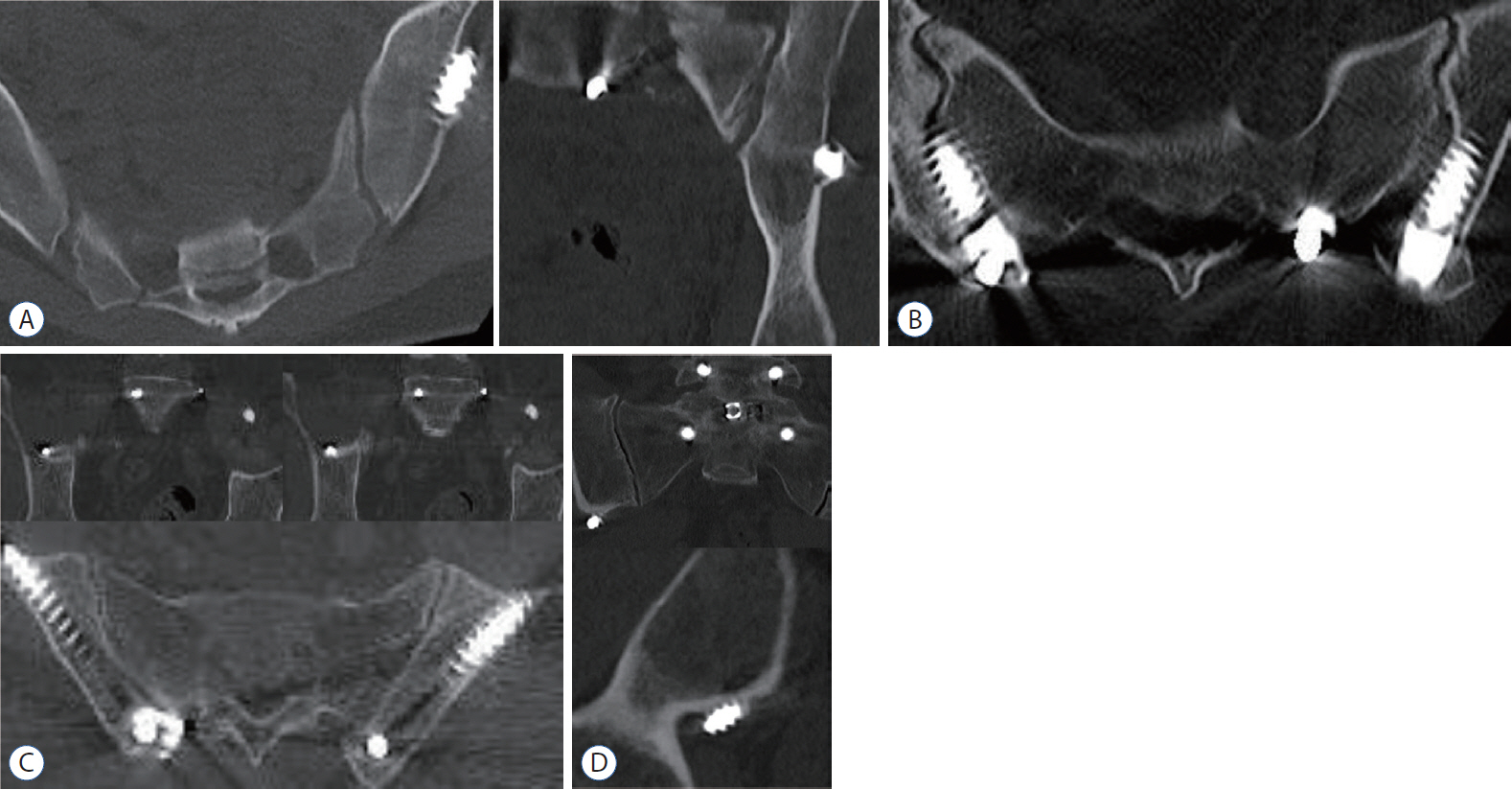
Fig. 2. A : Lateral wall violation, grade III (2.44 cm). B : Medial wall violation, grade III (2.38 cm). C : Superior wall violation, grade I (0.97 cm). D : Inferior wall violation, grade III (2.21 cm); none of the above cases needed revision surgery.
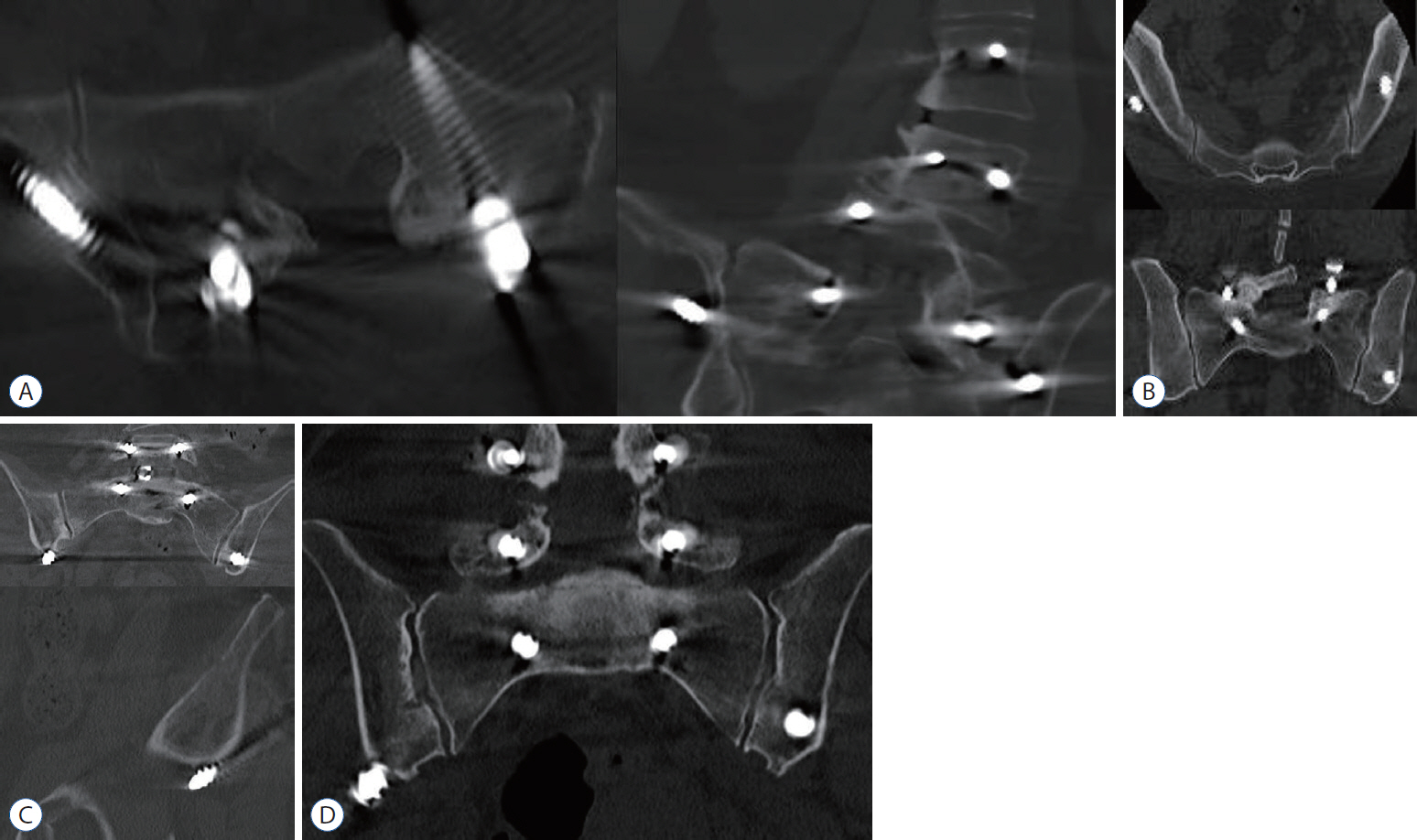
Fig. 3. A : Lateral wall violation, grade III (2.89 cm). B : Lateral wall violation, grade IV (3.12 cm). C : Inferior wall violation, grade III (2.32 cm). D : Inferior wall violation, grade IV (4.20 cm); all the above cases underwent revision surgery.
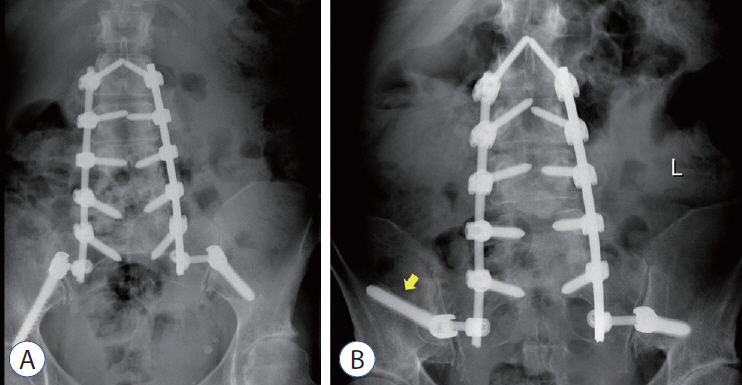
Fig. 4. Anterior-posterior radiographs of the spine in a 63-year-old woman with degenerative scoliosis. A : After the first surgery, both iliac screws were located above the sciatic notch on the image. However, the patient had severe pain in his right lower limb, and there was a grade IV screw breach on the right side; 4.20 cm inferior wall violation (Fig. 3D). B : Thus, we performed revisional surgery to replace the iliac screw toward a superior direction through another trajectory (yellow arrow).
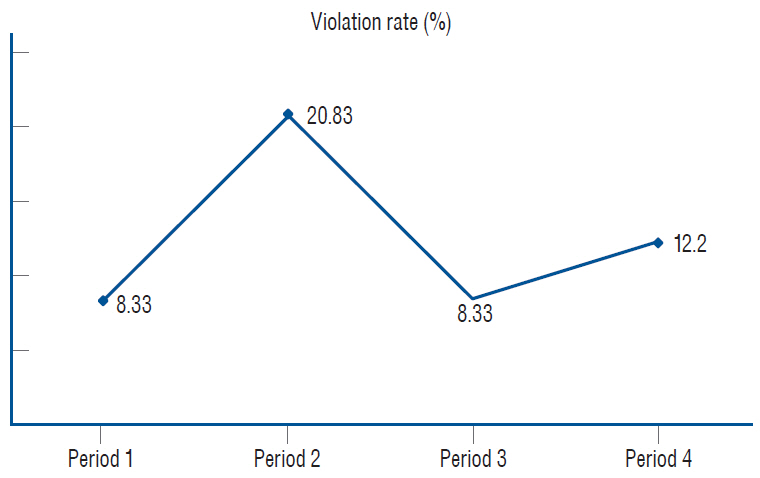
Fig. 5. The learning curve of iliac screw placement using the freehand technique (the violation rate is shown in the graph for each period).
Reference
-
References
1. Banno T, Hasegawa T, Yamato Y, Kobayashi S, Togawa D, Oe S, et al. Prevalence and risk factors of iliac screw loosening after adult spinal deformity surgery. Spine (Phila Pa 1976). 42:E1024–E1030. 2017.
Article2. Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am. 85:454–463. 2003.
Article3. Cho W, Mason JR, Smith JS, Shimer AL, Wilson AS, Shaffrey CI, et al. Failure of lumbopelvic fixation after long construct fusions in patients with adult spinal deformity: clinical and radiographic risk factors: clinical article. J Neurosurg Spine. 19:445–453. 2013.
Article4. DeWald RL, Arlet V, Carl AL, Obrien MF. Spinal deformities: the comprehensive text. Stuttgart: Georg Thieme Verlag;2003. p. 11–12.5. Fridley J, Fahim D, Navarro J, Wolinsky JP, Omeis I. Free-hand placement of iliac screws for spinopelvic fixation based on anatomical landmarks: technical note. Int J Spine Surg. 8:3. 2014.
Article6. Hsieh JC, Drazin D, Firempong AO, Pashman R, Johnson JP, Kim TT. Accuracy of intraoperative computed tomography image-guided surgery in placing pedicle and pelvic screws for primary versus revision spine surgery. Neurosurg Focus. 36:E2. 2014.
Article7. Jain A, Hassanzadeh H, Strike SA, Menga EN, Sponseller PD, Kebaish KM. Pelvic fixation in adult and pediatric spine surgery: historical perspective, indications, and techniques: AAOS exhibit selection. J Bone Joint Surg Am. 97:1521–1528. 2015.
Article8. Kebaish KM. Sacropelvic fixation: techniques and complications. Spine (Phila Pa 1976). 35:2245–2251. 2010.9. Kim YJ, Bridwell KH, Lenke LG, Cheh G, Baldus C. Results of lumbar pedicle subtraction osteotomies for fixed sagittal imbalance: a minimum 5-year follow-up study. Spine (Phila Pa 1976). 32:2189–2197. 2007.
Article10. Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD. Free hand pedicle screw placement in the thoracic spine: is it safe? Spine (Phila Pa 1976). 29:333–342. discussion 342. 2004.
Article11. Kuklo TR, Bridwell KH, Lewis SJ, Baldus C, Blanke K, Iffrig TM, et al. Minimum 2-year analysis of sacropelvic fixation and L5-S1 fusion using S1 and iliac screws. Spine (Phila Pa 1976). 26:1976–1983. 2001.
Article12. Lee CH, Hyun SJ, Kim YJ, Kim KJ, Jahng TA, Kim HJ. Accuracy of free hand pedicle screw installation in the thoracic and lumbar spine by a young surgeon: an analysis of the first consecutive 306 screws using computed tomography. Asian Spine J. 8:237–243. 2014.
Article13. O'Shaughnessy BA, Lenke LG, Bridwell KH, Cho W, Zebala LP, Chang MS, et al. Should symptomatic iliac screws be electively removed in adult spinal deformity patients fused to the sacrum? Spine (Phila Pa 1976). 37:1175–1181. 2012.14. Park JH, Jeon SR, Roh SW, Kim JH, Rhim SC. The safety and accuracy of freehand pedicle screw placement in the subaxial cervical spine: a series of 45 consecutive patients. Spine (Phila Pa 1976). 39:280–285. 2014.
Article15. Parker SL, McGirt MJ, Farber SH, Amin AG, Rick AM, Suk I, et al. Accuracy of free-hand pedicle screws in the thoracic and lumbar spine: analysis of 6816 consecutive screws. Neurosurgery. 68:170–178. discussion 178. 2011.
Article16. Perra JH. Techniques of instrumentation in long fusions to the sacrum. Orthop Clin North Am. 25:287–299. 1994.
Article17. Sandén B, Olerud C, Petrén-Mallmin M, Johansson C, Larsson S. The significance of radiolucent zones surrounding pedicle screws. Definition of screw loosening in spinal instrumentation. J Bone Joint Surg Br. 86:457–461. 2004.18. Schildhauer TA, McCulloch P, Chapman JR, Mann FA. Anatomic and radiographic considerations for placement of transiliac screws in lumbopelvic fixations. J Spinal Disord Tech. 15:199–205. discussion 205. 2002.
Article19. Shin JH, Hoh DJ, Kalfas IH. Iliac screw fixation using computer-assisted computer tomographic image guidance: technical note. Neurosurgery. 70:16–20. discussion 20. 2012.
Article20. Suk SI, Chung ER, Kim JH, Kim SS, Lee JS, Choi WK. Posterior vertebral column resection for severe rigid scoliosis. Spine (Phila Pa 1976). 30:1682–1687. 2005.
Article21. Suk SI, Chung ER, Lee SM, Lee JH, Kim SS, Kim JH. Posterior vertebral column resection in fixed lumbosacral deformity. Spine (Phila Pa 1976). 30:E703–E710. 2005.
Article22. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976). 31:303–308. 2006.
Article23. Wang MY, Berven SH. Lumbar pedicle subtraction osteotomy. Neurosurgery. 60:ONS140–ONS146. discussion ONS146. 2007.
Article24. Williams AL, Gornet MF, Burkus JK. CT evaluation of lumbar interbody fusion: current concepts. AJNR Am J Neuroradiol. 26:2057–2066. 2005.25. Wu JC, Huang WC, Tsai HW, Ko CC, Wu CL, Tu TH, et al. Pedicle screw loosening in dynamic stabilization: incidence, risk, and outcome in 126 patients. Neurosurg Focus. 31:E9. 2011.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Accuracy of Freehand versus Navigated Thoracolumbar Pedicle Screw Placement in Patients with Metastatic Tumors of the Spine
- Accuracy of Thoracolumbar Pedicle Screw Insertion Based on Routine Use of Intraoperative Imaging and Navigation
- Anatomical Evaluation of the Atlas and Analysis of Accuracy for Freehand C1 Screw Placement
- Freehand S2 Alar-Iliac Screw Placement Using K-Wire and Cannulated Screw: Technical Case Series
- Minimally Invasive Iliac Screw Insertion: Clinical Case Series and Technical Note
