Accuracy of Freehand versus Navigated Thoracolumbar Pedicle Screw Placement in Patients with Metastatic Tumors of the Spine
- Ramos RDLG
 1,2
1,2 - Echt M1,2
- Benton JA1
- Gelfand Y1,2
- Longo M1
- Yanamadala V1,2
- Yassari R1,2
- Affiliations
-
- 1Spine Research Group, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, USA
- 2Department of Neurological Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, USA
- KMID: 2508608
- DOI: http://doi.org/10.3340/jkns.2020.0001
Abstract
Objective
: To compare the accuracy and breach rates of freehand (FH) versus navigated (NV) pedicle screws in the thoracic and lumbar spine in patients with metastatic spinal tumors.
Methods
: A retrospective review of adult patients who underwent pedicle screw fixation in the thoracic or lumbar spine for metastatic spinal tumors between 2012 and 2018 was conducted. Breaches were assessed based on the Gertzbein and Robbins classification and only screws placed >4 mm outside of the pedicle wall (lateral or medial) were considered breached.
Results
: A total of 62 patients received 547 pedicle screws (average 8 per patient) – 34 patients received 298 pedicle screws in the FH group and 28 patients received 249 screws in the NV group. There were 40/547 breaches, corresponding to a breach and accuracy rate of 7.3% and 92.7%, respectively. The breach rate was 9.7% in the FH group and 4.4% in the NV group (chi-squared test, p=0.017); this corresponded to an accuracy rate of 90.3% and 95.6%, respectively. Only one patient from the overall cohort (in the FH group) required revision surgery due to a medial breach abutting the spinal cord (1.6% of all patients; 2.9% of FH patients); no patient suffered organ, vessel, or neurological injury from screw breaches.
Conclusion
: Navigated pedicle screw placement in patients with metastatic spinal tumors has a significantly higher radiographic accuracy compared to the FH technique. However, the revision surgery was low and no patient suffered from clinically-relevant breach. Navigation also offers the advantage of real-time localization of spinal tumors and aids in targeting and resection of these lesions.
Figure
-
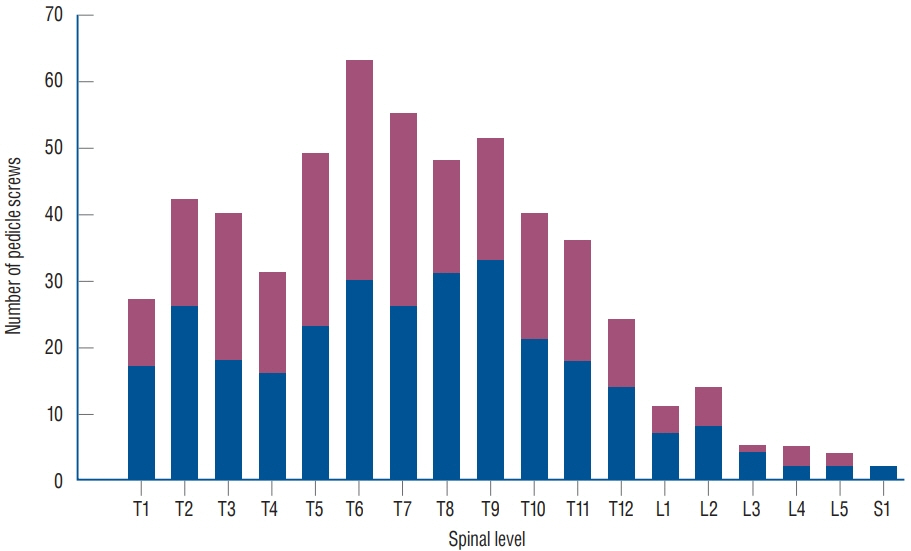
Fig. 1. Distribution of 547 pedicle screws placed in 62 patients with metastatic tumors of the spine. The distribution of screw placement by the freehand (blue) and navigated (red) technique was not significantly different (all p>0.05).
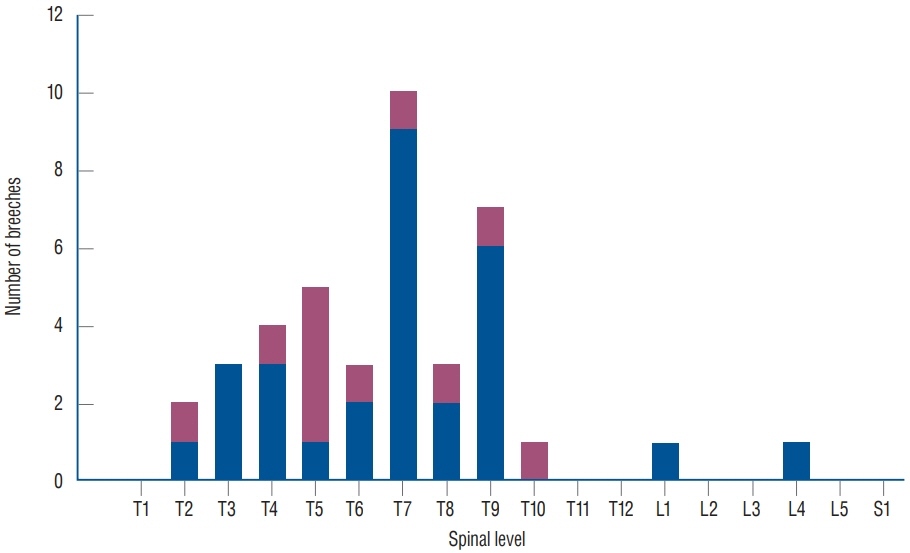
Fig. 2. Distribution of 47 pedicle screws breaches in 62 patients with metastatic tumors of the spine. The distribution of screw placement by the freehand (blue) and navigated (red) technique was not significantly different (all p>0.05).
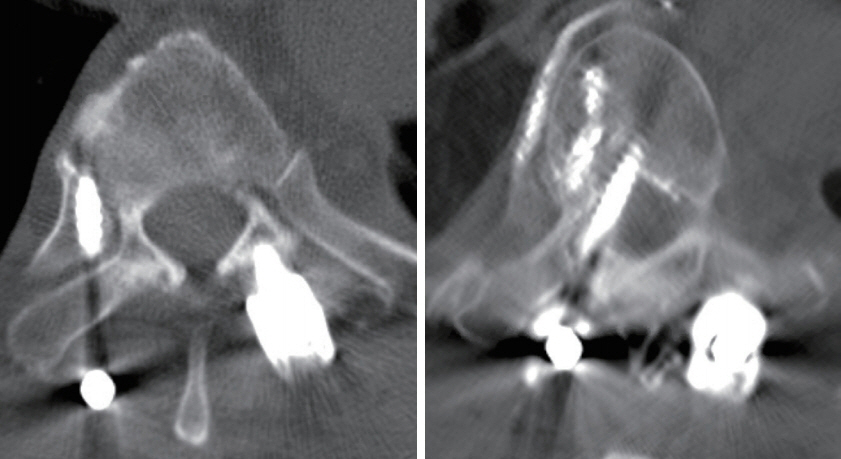
Fig. 3. Postoperative computed tomography scans showing examples of a lateral breach (left) and a medial breach (right). The patient with the medial breach was the only patient in our study who underwent revision due to close proximity to the spinal cord; no neurological sequelae occurred. This patient also had some extravasation of cement into the adjacent vasculature without any sequelae.
Reference
-
References
1. Arand M, Hartwig E, Kinzl L, Gebhard F. Spinal navigation in tumor surgery of the thoracic spine: first clinical results. Clin Orthop Relat Res. 399:211–218. 2002.
Article2. Brasiliense LB, Theodore N, Lazaro BC, Sayed ZA, Deniz FE, Sonntag VK, et al. Quantitative analysis of misplaced pedicle screws in the thoracic spine: how much pullout strength is lost?: presented at the 2009 Joint Spine Section Meeting. J Neurosurg Spine. 12:503–508. 2010.
Article3. Cho W, Cho SK, Wu C. The biomechanics of pedicle screw-based instrumentation. J Bone Joint Surg Br. 92:1061–1065. 2010.
Article4. duPleiss SJ, Hurlbert RJ. Pedicle screw fixation of the thoracic and lumbar spine. In : Dickman CA, Fehlings MG, Gokaslan ZL, editors. Spinal Cord and Spinal Column Tumors. New York: Thieme;2006. p. 587–598.5. Fourney DR, Abi-Said D, Lang FF, McCutcheon IE, Gokaslan ZL. Use of pedicle screw fixation in the management of malignant spinal disease: experience in 100 consecutive procedures. J Neurosurg. 94(1 Suppl):25–37. 2001.
Article6. Gautschi OP, Schatlo B, Schaller K, Tessitore E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management: a literature review of 35,630 pedicle screws. Neurosurg Focus. 31:E8. 2011.
Article7. Gelalis ID, Paschos NK, Pakos EE, Politis AN, Arnaoutoglou CM, Karageorgos AC, et al. Accuracy of pedicle screw placement: a systematic review of prospective in vivo studies comparing free hand, fluoroscopy guidance and navigation techniques. Eur Spine J. 21:247–255. 2012.
Article8. Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo. Spine (Phila Pa 1976). 15:11–14. 1990.
Article9. Innocenzi G, Bistazzoni S, D’Ercole M, Cardarelli G, Ricciardi F. Does navigation improve pedicle screw placement accuracy? Comparison between navigated and non-navigated percutaneous and open fixations. Acta Neurochir Suppl. 124:289–295. 2017.
Article10. Kakkos SK, Shepard AD. Delayed presentation of aortic injury by pedicle screws: report of two cases and review of the literature. J Vasc Surg. 47:1074–1082. 2008.
Article11. Karapinar L, Erel N, Ozturk H, Altay T, Kaya A. Pedicle screw placement with a free hand technique in thoracolumbar spine: is it safe? J Spinal Disord Tech. 21:63–67. 2008.
Article12. Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD. Free hand pedicle screw placement in the thoracic spine: is it safe? Spine (Phila Pa 1976). 29:333–342. discussion 342. 2004.
Article13. Kosmopoulos V, Schizas C. Pedicle screw placement accuracy: a metaanalysis. Spine (Phila Pa 1976). 32:E111–E120. 2007.14. Kotil K, Bilge T. Accuracy of pedicle and mass screw placement in the spine without using fluoroscopy: a prospective clinical study. Spine J. 8:591–596. 2008.
Article15. Krag MH, Beynnon BD, Pope MH, Frymoyer JW, Haugh LD, Weaver DL. An internal fixator for posterior application to short segments of the thoracic, lumbar, or lumbosacral spine. Design and testing. Clin Orthop Relat Res. 203:75–98. 1986.
Article16. Lehman RA Jr, Kang DG, Lenke LG, Gaume RE, Paik H. The ventral lamina and superior facet rule: a morphometric analysis for an ideal thoracic pedicle screw starting point. Spine J. 14:137–144. 2014.
Article17. Luther N, Iorgulescu JB, Geannette C, Gebhard H, Saleh T, Tsiouris AJ, et al. Comparison of navigated versus non-navigated pedicle screw placement in 260 patients and 1434 screws: screw accuracy, screw size, and the complexity of surgery. J Spinal Disord Tech. 28:E298–E303. 2015.18. Moussazadeh N, Rubin DG, McLaughlin L, Lis E, Bilsky MH, Laufer I. Short-segment percutaneous pedicle screw fixation with cement augmentation for tumor-induced spinal instability. Spine J. 15:1609–1617. 2015.
Article19. Nasser R, Drazin D, Nakhla J, Al-Khouja L, Brien E, Baron EM, et al. Resection of spinal column tumors utilizing image-guided navigation: a multicenter analysis. Neurosurg Focus. 41:E15. 2016.
Article20. Parker SL, McGirt MJ, Farber SH, Amin AG, Rick AM, Suk I, et al. Accuracy of free-hand pedicle screws in the thoracic and lumbar spine: analysis of 6816 consecutive screws. Neurosurgery. 68:170–178. discussion 178. 2011.
Article21. Rajasekaran S, Kamath V, Shetty AP. Intraoperative Iso-C three-dimensional navigation in excision of spinal osteoid osteomas. Spine (Phila Pa 1976). 33:E25–E29. 2008.
Article22. Shin BJ, James AR, Njoku IU, Härtl R. Pedicle screw navigation: a systematic review and meta-analysis of perforation risk for computernavigated versus freehand insertion. J Neurosurg Spine. 17:113–122. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic spine systems: overcoming surgeon experience in pedicle screw accuracy: a prospective study
- Learning Curve for Robot-Assisted Percutaneous Pedicle Screw Placement in Thoracolumbar Surgery
- Radiologic Evaluation of Proper Pedicle Screw Placement after Pedicle Screw Fixation in Degenerative Lumbar Disc Disease
- The Accuracy and Safety of a Pedicle Screw Using the Freehand Technique in Minimally Invasive Scoliosis Surgery
- Postoperative Assessment of Pedicle Screws and Management of Breaches: A Survey among Canadian Spine Surgeons and a New Scoring System
