Freehand S2 Alar-Iliac Screw Placement Using K-Wire and Cannulated Screw: Technical Case Series
- Affiliations
-
- 1Department of Neurosurgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
- 2Department of Neurosurgery, Spine Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. hyunsj@snu.ac.kr
- KMID: 2403526
- DOI: http://doi.org/10.3340/jkns.2016.1212.008
Abstract
OBJECTIVE
Among the various sacropelvic fixation methods, S2 alar-iliac (S2AI) screw fixation has several advantages compared to conventional iliac wing screw. However, the placement of S2AI screw still remains a challenge. The purpose of this study was to describe a novel technique of free hand S2AI screw insertion using a K-wire and cannulated screw, and to evaluate the accuracy of the technique.
METHODS
S2AI screw was inserted by free hand technique in sixteen consecutive patients without any fluoroscopic guidance. The gearshift was advanced to make a pilot hole passing through the sacroiliac joint and directing the anterior inferior iliac spine. A K-wire was placed through the pilot hole. After introducing a cannulated tapper along with the K-wire, a cannulated S2AI screw was installed over the K-wire.
RESULTS
Thirty-three S2AI screws were placed in sixteen consecutive patients. Thirty-two screws were cannulated screws, and one screw was a conventional non-cannulated screw. Thirty out of 32 (93.8%) cannulated screws were accurately positioned, whereas two cannulated screws and one non-cannulated screw violated lateral cortex of the ilium.
CONCLUSION
The technique using K-wire and cannulated screw can provide accurate placement of free hand S2AI screw.
MeSH Terms
Figure
-

Fig. 1 A : The gearshift is initially pointed dorsally to avoid anterior wall violation of the pelvic bone. After crossing the sacroiliac joint, the tip is turned ventrally. B : After the pilot hole is created and verified as intraosseous, K-wire is placed through the hole. C : Tapping is performed with a cannulated tap along with the K-wire. D : Cannulated S2 alar-iliac screw is inserted over the K-wire in the same manner.

Fig. 2 Anteroposterior and lateral plain radiographs demonstrate S2 alar-iliac (S2AI) screw insertion using cannulated screws. Note the radiolucent line inside the screw (arrows). Two S2AI screws are accurately placed.
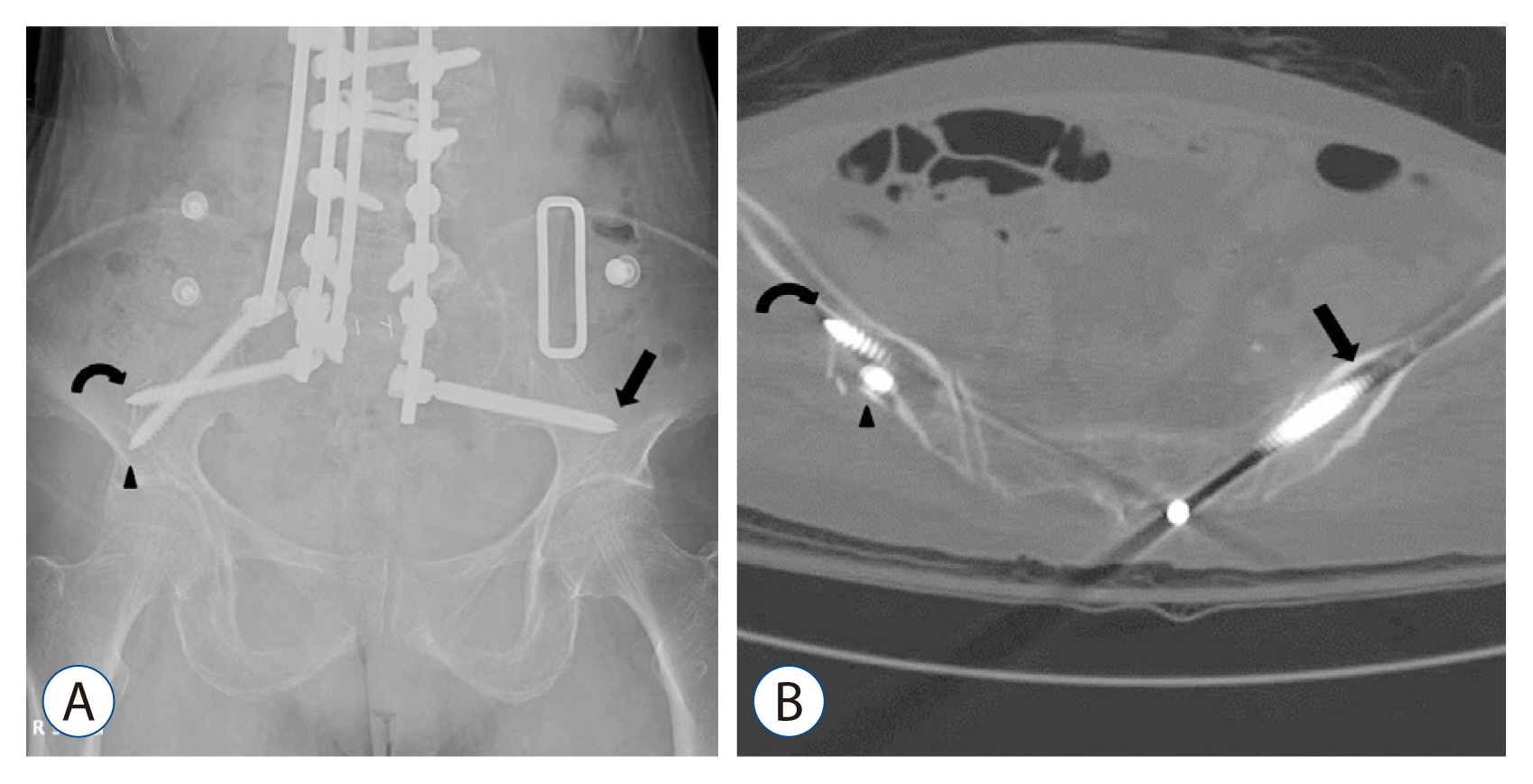
Fig. 3 A : Anteroposterior plain radiograph of Patient 3. A cannulated S2 alar-iliac (S2AI) screw (arrow) was inserted on the left side, whereas conventional non-cannulated S2AI screw (curved arrow) was inserted on the right side with the additional iliac wing screw (arrowhead). B : Computed tomographic axial image of the same patient demonstrates cortical violation of the lateral ilium by the conventional non-cannulated S2AI screw (curved arrow) and iliac wing screw (arrowhead). Cannulated S2AI screw (arrow) was accurately positioned on the left side.
Cited by 2 articles
-
Surgical Impacts of Metastatic Non-small Cell Lung Cancer to the Thoracic and Lumbar Spine
Jong-myung Jung, Seung-Jae Hyun, Ki-Jeong Kim
J Korean Med Sci. 2021;36(7):e52. doi: 10.3346/jkms.2021.36.e52.Radiographic and Clinical Outcomes Following Pedicle Subtraction Osteotomy : Minimum 2-Year Follow-Up Data
Ho Yong Choi, Seung-Jae Hyun, Ki-Jeong Kim, Tae-Ahn Jahng, Hyun-Jib Kim
J Korean Neurosurg Soc. 2020;63(1):99-107. doi: 10.3340/jkns.2018.0170.
Reference
-
References
1. Balderston RA, Winter RB, Moe JH, Bradford DS, Lonstein JE. Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine (Phila Pa 1976). 11:824–829. 1986.
Article2. Chang TL, Sponseller PD, Kebaish KM, Fishman EK. Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation versus traditional iliac fixation. Spine (Phila Pa 1976). 34:436–440. 2009.3. Emami A, Deviren V, Berven S, Smith JA, Hu SS, Bradford DS. Outcome and complications of long fusions to the sacrum in adult spine deformity: luque-galveston, combined iliac and sacral screws, and sacral fixation. Spine (Phila Pa 1976). 27:776–786. 2002.
Article4. Erkan S, Hsu B, Wu C, Mehbod AA, Perl J, Transfeldt EE. Alignment of pedicle screws with pilot holes: can tapping improve screw trajectory in thoracic spines? Eur Spine J. 19:71–77. 2010.
Article5. Hyun SJ, Kim KJ, Jahng TA, Kim HJ. Efficiency of lead aprons in blocking radiation - how protective are they? Heliyon. 2:e00117. 2016.
Article6. Jain A, Hassanzadeh H, Strike SA, Menga EN, Sponseller PD, Kebaish KM. Pelvic fixation in adult and pediatric spine surgery: historical perspective, indications, and techniques: AAOS exhibit selection. J Bone Joint Surg Am. 97:1521–1528. 2015.
Article7. Kebaish KM. Sacropelvic fixation: techniques and complications. Spine (Phila Pa 1976). 35:2245–2251. 2010.8. Kim YJ, Bridwell KH, Lenke LG, Cho KJ, Edwards CC 2nd, Rinella AS. Pseudarthrosis in adult spinal deformity following multisegmental instrumentation and arthrodesis. J Bone Joint Surg Am. 88:721–728. 2006.
Article9. Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD. Free hand pedicle screw placement in the thoracic spine: is it safe? Spine (Phila Pa 1976). 29:333–342. discussion 342. 2004.
Article10. Kuklo TR, Bridwell KH, Lewis SJ, Baldus C, Blanke K, Iffrig TM, et al. Minimum 2-year analysis of sacropelvic fixation and L5-S1 fusion using S1 and iliac screws. Spine (Phila Pa 1976). 26:1976–1983. 2001.
Article11. Lehman RA, Potter BK, Kuklo TR, Chang AS, Polly DW, Shawen SB, et al. Probing for thoracic pedicle screw tract violation(s): is it valid? J Spinal Disord Tech. 17:277–283. 2004.12. Martin CT, Witham TF, Kebaish KM. Sacropelvic fixation: two case reports of a new percutaneous technique. Spine (Phila Pa 1976). 36:E618–E621. 2011.13. Nottmeier EW, Pirris SM, Balseiro S, Fenton D. Three-dimensional image-guided placement of S2 alar screws to adjunct or salvage lumbosacral fixation. Spine J. 10:595–601. 2010.
Article14. O’Brien JR, Yu WD, Bhatnagar R, Sponseller P, Kebaish KM. An anatomic study of the S2 iliac technique for lumbopelvic screw placement. Spine (Phila Pa 1976). 34:E439–E442. 2009.
Article15. Park JH, Hyun SJ, Kim KJ, Jahng TA. Free hand insertion technique of S2 sacral alar-iliac screws for spino-pelvic fixation: technical note, acadaveric study. J Korean Neurosurg Soc. 58:578–581. 2015.
Article16. Schwend RM, Sluyters R, Najdzionek J. The pylon concept of pelvic anchorage for spinal instrumentation in the human cadaver. Spine (Phila Pa 1976). 28:542–547. 2003.
Article17. Sponseller PD, Zimmerman RM, Ko PS, Pull Ter Gunne AF, Mohamed AS, Chang TL, et al. Low profile pelvic fixation with the sacral alar iliac technique in the pediatric population improves results at two-year minimum follow-up. Spine (Phila Pa 1976). 35:1887–1892. 2010.
Article18. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976). 31:303–308. 2006.
Article19. Wind JJ, Burke LM, Kurtom KH, Roberti F, O’Brien JR. Minimally invasive lumbopelvic instrumentation for traumatic sacrolisthesis in an elderly patient. Eur Spine J 21 Suppl. 4:S549–S553. 2012.
Article20. Zhu F, Bao HD, Yuan S, Wang B, Qiao J, Zhu ZZ, et al. Posterior second sacral alar iliac screw insertion: anatomic study in a Chinese population. Eur Spine J. 22:1683–1689. 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is S1 Alar Iliac Screw a Feasible Option for Lumbosacral Fixation?: A Technical Note
- Free Hand Insertion Technique of S2 Sacral Alar-Iliac Screws for Spino-Pelvic Fixation: Technical Note, Acadaveric Study
- Lumbosacral Fixation Using the Diagonal S2 Screw for Long Fusion in Degenerative Lumbar Deformity: Technical Note Involving 13 Cases
- Accuracy Analysis of Iliac Screw Using Freehand Technique in Spinal Surgery : Relation between Screw Breach and Revision Surgery
- A Computed Tomography-Based Assessment of the Anatomical Parameters Concerning S2-Alar Iliac Screw Insertion Using “Safe Trajectory Method” in Indian Population
