Yeungnam Univ J Med.
2020 Jan;37(1):54-58. 10.12701/yujm.2019.00276.
Community-acquired Achromobacter xylosoxidans infection presenting as a cavitary lung disease in an immunocompetent patient
- Affiliations
-
- 1Republic of Korea Defence Intelligence Command, Anyang, Korea
- 2Department of Laboratory Medicine, Cheju Halla General Hospital, Jeju, Korea
- 3Department of Internal Medicine, Cheju Halla General Hospital, Jeju, Korea
- KMID: 2501408
- DOI: http://doi.org/10.12701/yujm.2019.00276
Abstract
- Achromobacter xylosoxidans is a gram-negative bacterium that can oxidize xylose. It is commonly found in contaminated soil and water but does not normally infect immunocompetent humans. We report a case of a cavitary lung lesion associated with community-acquired A. xylosoxidans infection, which mimicked pulmonary tuberculosis or lung cancer in an immunocompetent man. The patient was hospitalized due to hemoptysis, and chest computed tomography (CT) revealed a cavitary lesion in the superior segment of the left lower lobe. We performed bronchoscopy and bronchial washing, and subsequent bacterial cultures excluded pulmonary tuberculosis and identified A. xylosoxidans. We performed antibiotic sensitivity testing and treated the patient with a 6-week course of amoxicillin/clavulanate. After 2 months, follow-up chest CT revealed complete resolution of the cavitary lesion.
Keyword
Figure
-
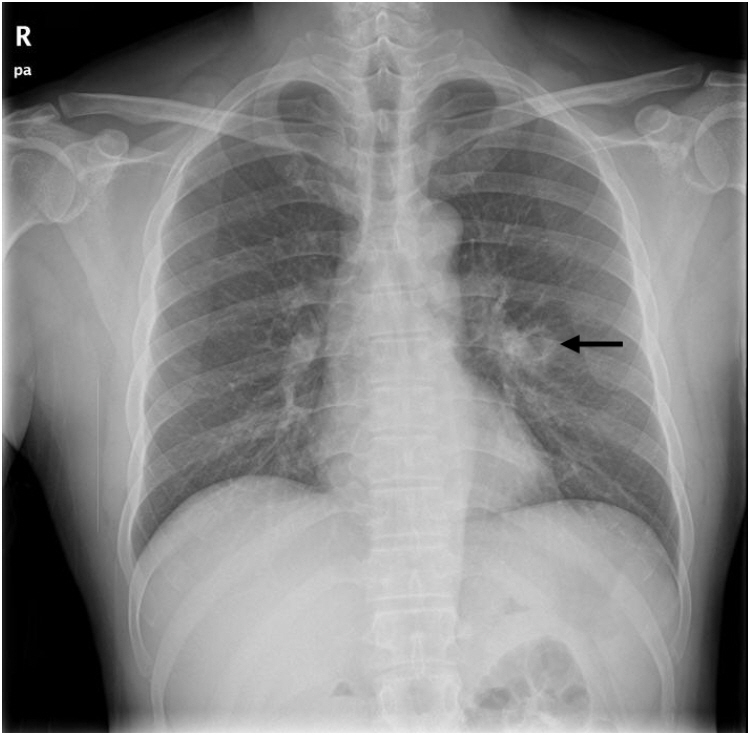
Fig. 1. Chest radiography reveals a cavitary lesion (arrow) in the left lung.
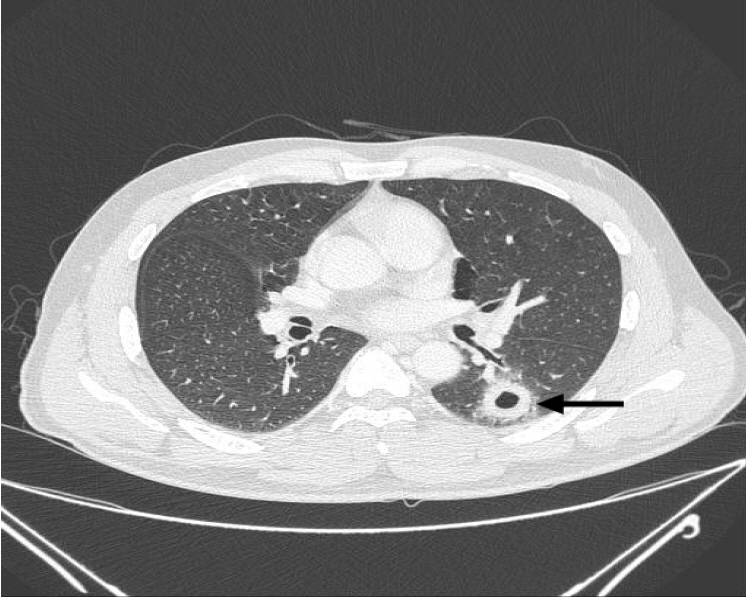
Fig. 2. Chest computed tomography reveals a smooth internal margin of a cavitary mass (approximate size, 2.4 cm) with surrounding reticulonodular opacities (arrow) in the superior segment of the left lower lobe.

Fig. 3. Bronchoscopy reveals mild stenosis (arrow) in the lateralis bronchus orifice of the superior segment of the left lower lobe.

Fig. 4. Chest computed tomography after 2 months reveals complete resolution of the cavitary lesion in the superior segment of the left lower lobe.
Reference
-
References
1. Yabuuchi E, Yano I, Goto S, Tanimura E, Ito T, Ohyama A. Description of Achromobacter xylosoxidans Yabuuchi and Ohyama 1971. Int J Syst Bacteriol. 1974; 24:470–7.2. Yang YW, Kang YA, Lee SH, Lee SM, Yoo CG, Kim YW, et al. Aetiologies and predictors of pulmonary cavities in South Korea. Int J Tuberc Lung Dis. 2007; 11:457–62.3. Lee JH, Nam DH, Kim DH, Kim SH, Kim HN, Han CH, et al. Two cases of pulmonary infection due to A. xylosoxidans infection in an immunocompentent patient. Tuberc Respir Dis. 2008; 64:33–8.
Article4. Yabuuchi E, Oyama A. Achromobacter xylosoxidans n. sp. from human ear discharge. Jpn J Microbiol. 1971; 15:477–81.5. Claassen SL, Reese JM, Mysliwiec V, Mahlen SD. Achromobacter xylosoxidans infection presenting as a pulmonary nodule mimicking cancer. J Clin Microbiol. 2011; 49:2751–4.
Article6. De Baets F, Schelstraete P, Van Daele S, Haerynck F, Vaneechoutte M. Achromobacter xylosoxidans in cystic fibrosis: prevalence and clinical relevance. J Cyst Fibros. 2007; 6:75–8.7. Saiman L, Chen Y, Tabibi S, San Gabriel P, Zhou J, Liu Z, et al. Identification and antimicrobial susceptibility of Alcaligenes xylosoxidans isolated from patients with cystic fibrosis. J Clin Microbiol. 2001; 39:3942–5.
Article8. Kim NR, Han J. Pathologic review of cystic and cavitary lung diseases. Korean J Pathol. 2012; 46:407–14.
Article9. Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008; 21:305–33.
Article10. Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005; 72:1253–60.11. Gómez-Cerezo J, Suárez I, Ríos JJ, Peña P, García de Miguel MJ, de José M, et al. Achromobacter xylosoxidans bacteremia: a 10-year analysis of 54 cases. Eur J Clin Microbiol Infect Dis. 2003; 22:360–3.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Septic Shock caused by Achromobacter xylosoxidans in an Immunocompetent Female Patient after Extracorporeal Shock Wave Lithotripsy for a Ureteral Stone
- Achromobacter xylosoxidans Infection Following Total Knee Arthroplasty
- A Case of Achromobacter Xylosoxidans Keratitis
- Achromobacter xylosoxidans Bacteremia in a Child with Neutropenia
- A Case of Peritonitis Due to Achromobacter xylosoxidans subsp. xylosoxidans in a Patient Undergoing Continuous Ambulatory Peritoneal Dialysis (CAPD)
