Update of endoscopic management of Crohn’s disease strictures
- Affiliations
-
- 1Interventional IBD Center, Columbia University Irving Medical Center-New York Presbyterian Hospital, New York, NY, USA
- KMID: 2501362
- DOI: http://doi.org/10.5217/ir.2019.09158
Abstract
- One of the most common complications of Crohn’s disease (CD) is the formation of strictures. Endoscopy plays a vital role not only in the diagnosis, differential diagnosis, and disease monitoring of CD, but also the delivery of effective treatment. The purpose of this review is to update the endoscopic management of strictures in CD. Endoscopic therapy has provided minimally invasive treatment for CD. Commonly used endoscopic treatment modalities include balloon dilation, endoscopic stricturotomy, endoscopic strictureplasty, and endoscopic stenting. The pros and cons of these endoscopic treatment modalities are discussed.
Keyword
Figure
-
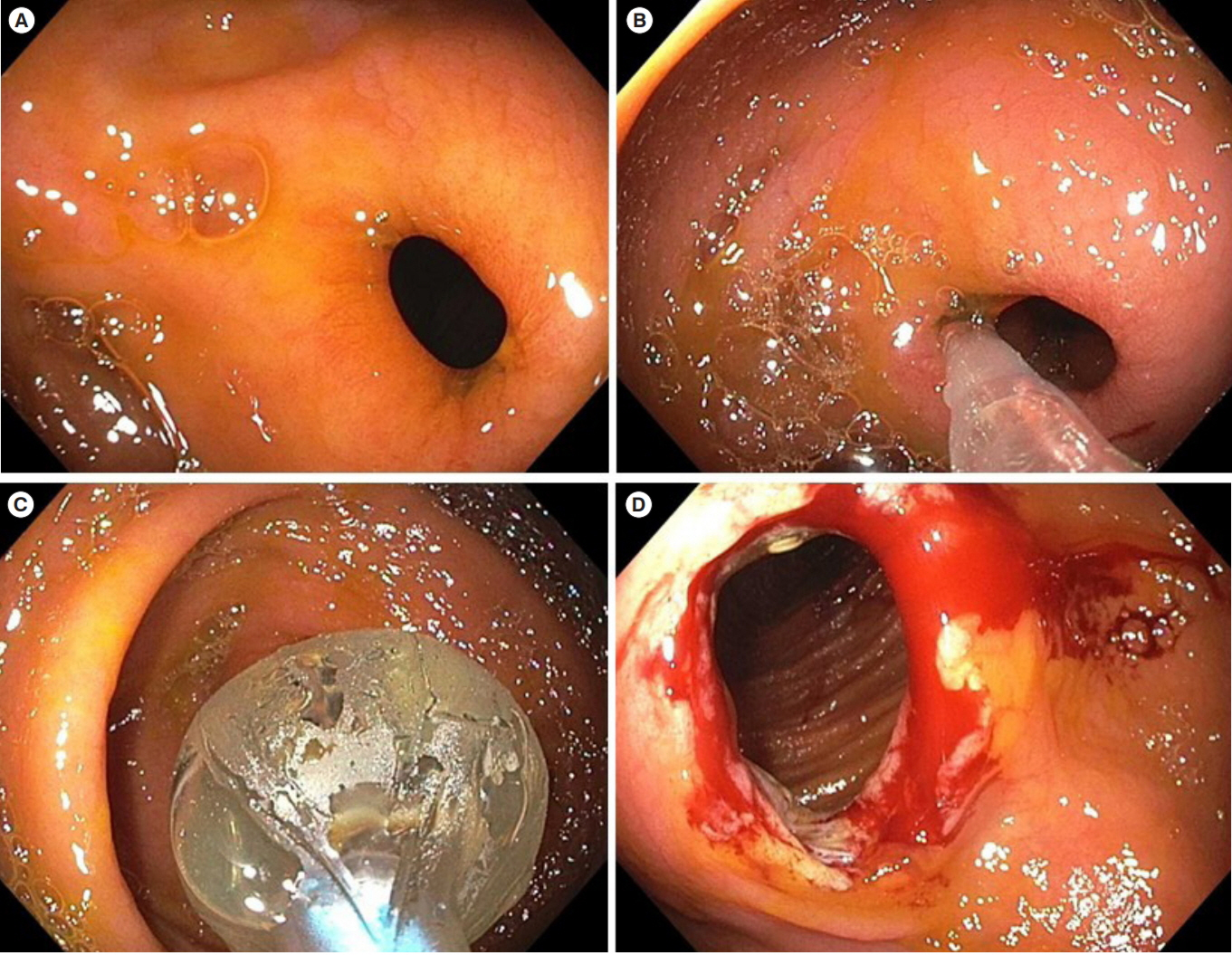
Fig. 1. Antegrade endoscopic balloon dilation of an ileocolonic anastomosis stricture in CD. (A) The tight, nonulcerated stricture at the anastomosis. (B, C) Balloon dilation of the stricture prior to the passage of the scope. (D) Post-dilation appearance of the stricture with some bleeding.
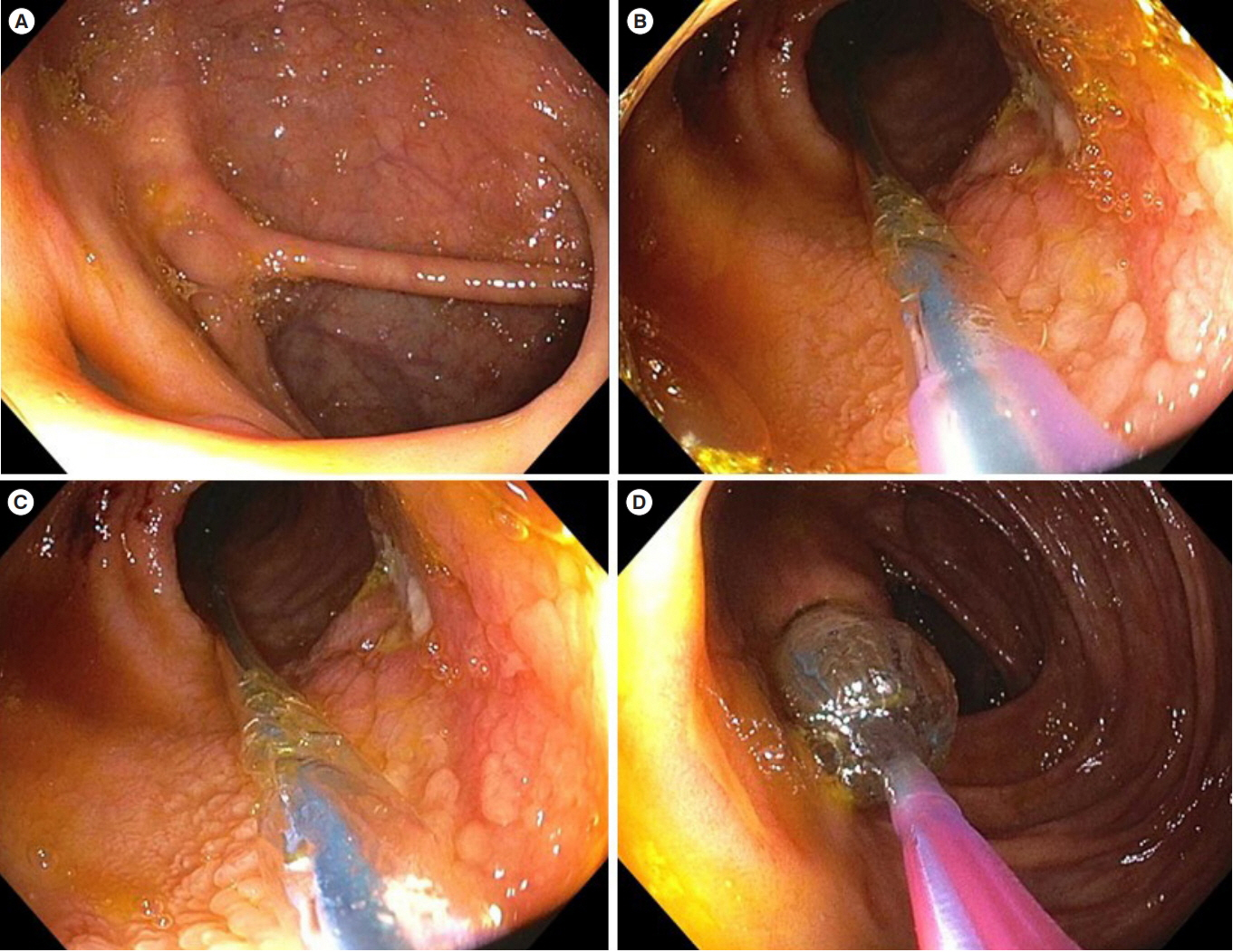
Fig. 2. Retrograde endoscopic balloon dilation of an ileocecal valve stricture in CD. (A) The nonulcerated stricture at the ileocecal valve which was traversable to a pediatric colonoscope. (B, C) Passage of endoscope through the stricture and advancement of balloon sheath. (D) Withdrawal of the scope along with advanced balloon sheath and subsequent insufflation of the balloon.
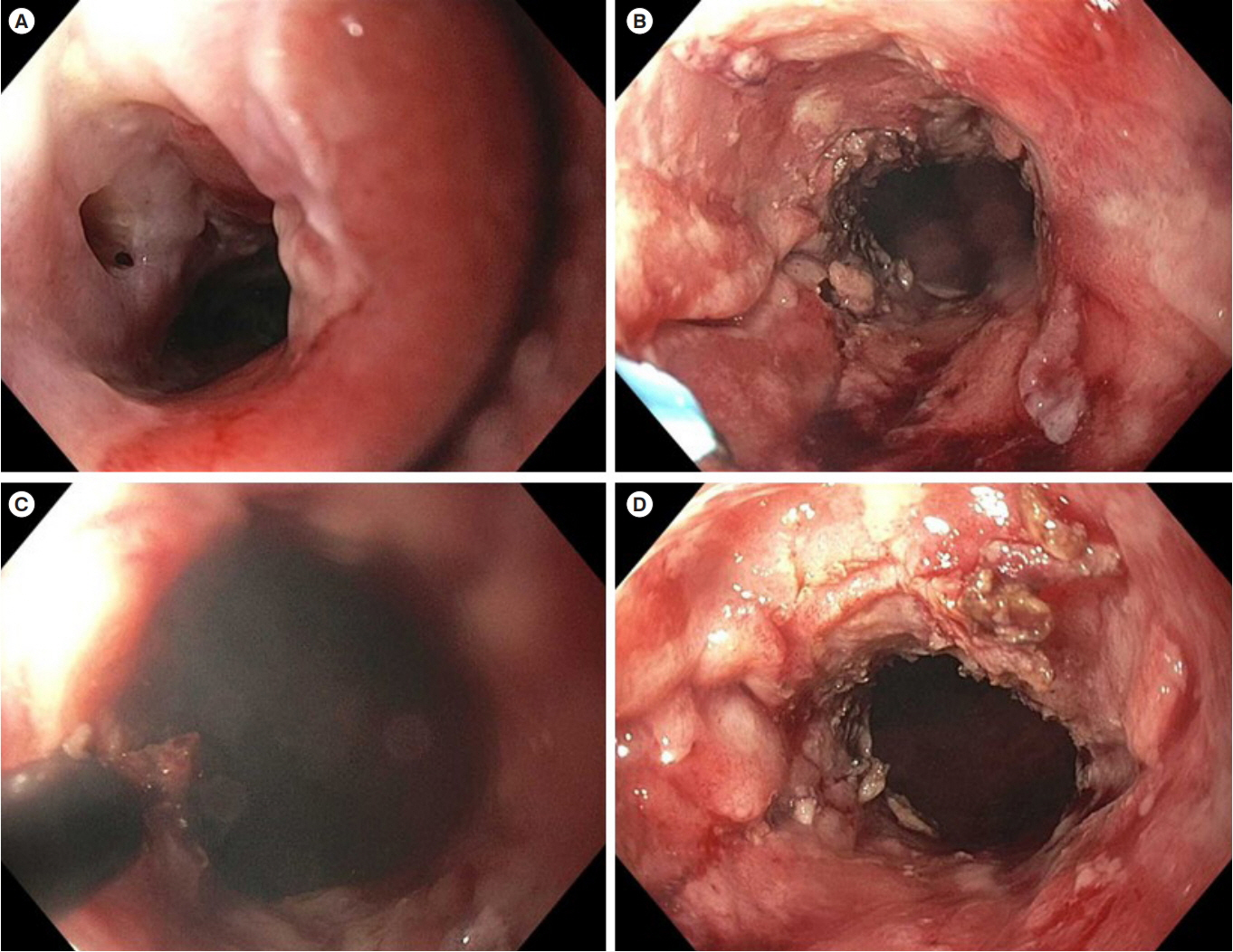
Fig. 3. Endoscopic stricturotomy of a long anorectal stricture in CD. (A) The 6-cm long tight ulcerated stricture resulting from the disease and previous repeated endoscopic balloon and bougie dilations. (B) Stricturotomy with a needle knife. (C) Stricturotomy with an insulated-tip knife. (D) Posttreatment appearance of the stricture.

Fig. 4. Endoscopic strictureplasty of an ileocolonic anastomotic stricture in CD. (A) The short, ulcerated stricture with dislodged staples at the anastomosis. (B, C) Endoscopic electroincision with a needle knife. (D) Placement of endoclips to the incised stricture as spacers.
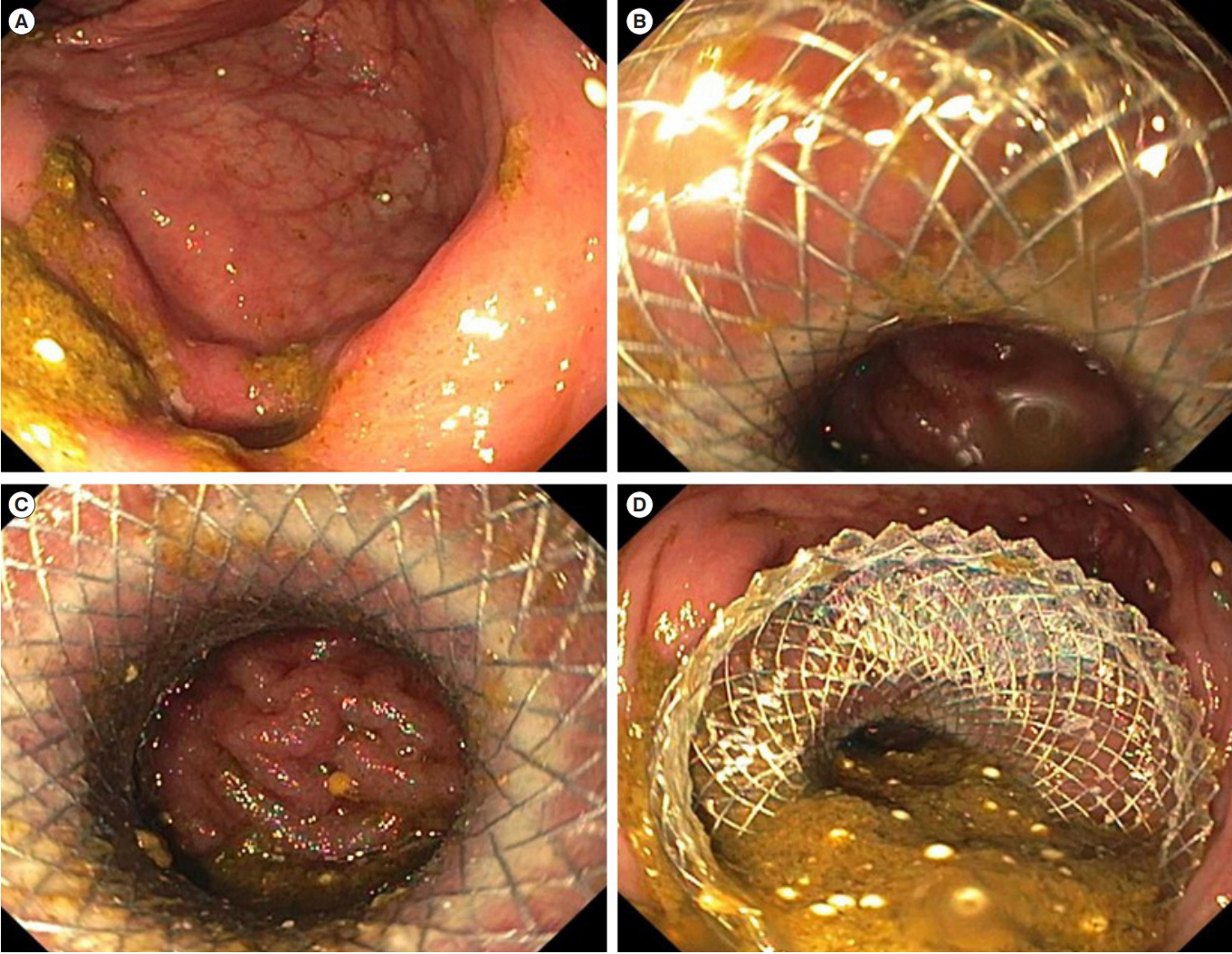
Fig. 5. Endoscopic stenting of a short ileocolonic anastomotic stricture in CD. (A) The tight, short anastomosis stricture. (B-D) Placement of a 22×10 mm lumen-opposing metal stent.
Reference
-
1. East JE, Brooker JC, Rutter MD, Saunders BP. A pilot study of intrastricture steroid versus placebo injection after balloon dilatation of Crohn’s strictures. Clin Gastroenterol Hepatol. 2007; 5:1065–1069.
Article2. Di Nardo G, Oliva S, Passariello M, et al. Intralesional steroid injection after endoscopic balloon dilation in pediatric Crohn’s disease with stricture: a prospective, randomized, doubleblind, controlled trial. Gastrointest Endosc. 2010; 72:1201–1208.
Article3. Li Y, Stocchi L, Shen B, Liu X, Remzi FH. Salvage surgery after failure of endoscopic balloon dilatation versus surgery first for ileocolonic anastomotic stricture due to recurrent Crohn’s disease. Br J Surg. 2015; 102:1418–1425.
Article4. Shivashankar R, Edakkanambeth Varayil J, Scott Harmsen W, et al. Outcomes of endoscopic therapy for luminal strictures in Crohn’s disease. Inflamm Bowel Dis. 2018; 24:1575–1581.
Article5. Scimeca D, Mocciaro F, Cottone M, et al. Efficacy and safety of endoscopic balloon dilation of symptomatic intestinal Crohn’s disease strictures. Dig Liver Dis. 2011; 43:121–125.
Article6. Gustavsson A, Magnuson A, Blomberg B, Andersson M, Halfvarson J, Tysk C. Endoscopic dilation is an efficacious and safe treatment of intestinal strictures in Crohn’s disease. Aliment Pharmacol Ther. 2012; 36:151–158.
Article7. Mueller T, Rieder B, Bechtner G, Pfeiffer A. The response of Crohn’s strictures to endoscopic balloon dilation. Aliment Pharmacol Ther. 2010; 31:634–639.
Article8. Lee HW, Park SJ, Jeon SR, et al. Long-term outcomes of endoscopic balloon dilation for benign strictures in patients with inflammatory bowel disease. Gut Liver. 2018; 12:530–536.
Article9. Lian L, Stocchi L, Shen B, et al. Prediction of need for surgery after endoscopic balloon dilation of ileocolic anastomotic stricture in patients with Crohn’s disease. Dis Colon Rectum. 2015; 58:423–430.
Article10. Atreja A, Aggarwal A, Dwivedi S, et al. Safety and efficacy of endoscopic dilation for primary and anastomotic Crohn’s disease strictures. J Crohns Colitis. 2014; 8:392–400.
Article11. Chen M, Shen B. Comparable short- and long-term outcomes of colonoscopic balloon dilation of Crohn’s disease and benign non-Crohn’s disease strictures. Inflamm Bowel Dis. 2014; 20:1739–1746.
Article12. Lian L, Stocchi L, Remzi FH, Shen B. Comparison of endoscopic dilation vs surgery for anastomotic stricture in patients with Crohn’s disease following ileocolonic resection. Clin Gastroenterol Hepatol. 2017; 15:1226–1231.
Article13. Morar PS, Faiz O, Warusavitarne J, et al. Systematic review with meta-analysis: endoscopic balloon dilatation for Crohn’s disease strictures. Aliment Pharmacol Ther. 2015; 42:1137–1148.
Article14. Axelrad JE, Lichtiger S, Sethi A. Treatment of Crohn’s disease anastomotic stricture with a lumen-apposing metal stent. Clin Gastroenterol Hepatol. 2018; 16:A25–A26.15. Bettenworth D, Gustavsson A, Atreja A, et al. A pooled analysis of efficacy, safety, and long-term outcome of endoscopic balloon dilation therapy for patients with stricturing Crohn’s disease. Inflamm Bowel Dis. 2017; 23:133–142.
Article16. Lan N, Stocchi L, Ashburn JH, et al. Outcomes of endoscopic balloon dilation vs surgical resection for primary ileocolic strictures in patients with Crohn’s disease. Clin Gastroenterol Hepatol. 2018; 16:1260–1267.
Article17. Klag T, Wehkamp J, Goetz M. Endoscopic balloon dilation for Crohn’s disease-associated strictures. Clin Endosc. 2017; 50:429–436.
Article18. Lan N, Shen B. Endoscopic stricturotomy with needle knife in the treatment of strictures from inflammatory bowel disease. Inflamm Bowel Dis. 2017; 23:502–513.
Article19. Lan N, Shen B. Endoscopic stricturotomy versus balloon dilation in the treatment of anastomotic strictures in Crohn’s disease. Inflamm Bowel Dis. 2018; 24:897–907.
Article20. Lan N, Shen B. Endoscopic stricturotomy vs surgical re-resection in the treatment of anastomotic strictures in Crohn’s disease. Gastrointest Endosc. 2018; 87:AB237–AB238.21. Karstensen JG, Christensen KR, Brynskov J, Rønholt C, Vilmann P, Hendel J. Biodegradable stents for the treatment of bowel strictures in Crohn’s disease: technical results and challenges. Endosc Int Open. 2016; 4:E296–E300.
Article22. El Ouali S, Kessler H, Shen B. Self-expandable metal stent in the treatment of refractory long pouch inlet stricture. Inflamm Bowel Dis. 2019; 25:e13–e14.
Article23. Loras C, Pérez-Roldan F, Gornals JB, et al. Endoscopic treatment with self-expanding metal stents for Crohn’s disease strictures. Aliment Pharmacol Ther. 2012; 36:833–839.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current status of endoscopic balloon dilation for Crohn's disease
- Endoscopic Balloon Dilation for Crohn’s Disease-Associated Strictures
- Differentiation of fibrotic and inflammatory component of Crohn’s disease-associated strictures
- Fibrostenotic strictures in Crohn’s disease
- A Case of Benign Colonic Stricture Treated by Therapeutic Balloon Dilatation in Ulcerative Colitis
