Endoscopic Balloon Dilation for Crohn’s Disease-Associated Strictures
- Affiliations
-
- 1Department of Internal Medicine I (Gastroenterology, Hepatology, Infectious Diseases), University Hospital Tübingen, Tübingen, Germany. martin.goetz@med.uni-tuebingen.de
- KMID: 2394742
- DOI: http://doi.org/10.5946/ce.2017.147
Abstract
- Management of intestinal strictures associated with Crohn's disease (CD) is clinically challenging despite advanced medical therapy directed toward mucosal healing to positively influence the natural course of CD-associated complications. Although medical therapy is available for inflammatory strictures, therapy of fibrostenotic strictures is the domain of surgery and endoscopy. Endoscopic balloon dilation (EBD) has been recognized as a well-established first-line procedure in terms of safety and efficacy. Although surgery is a valuable treatment modality for the management of CD-related strictures, EBD can help prevent multiple surgical interventions, which might in the long-term lead to a risk of short bowel syndrome. In this review we discuss requirements, techniques, safety, short- and long-term outcomes, as well as combinations of this procedure with surgical and medical treatment in CD-associated intestinal strictures.
Figure
-

Fig. 1. Antegrade balloon dilation (from left to right). A balloon is gently introduced into the stricture followed by hydrostatic dilation.
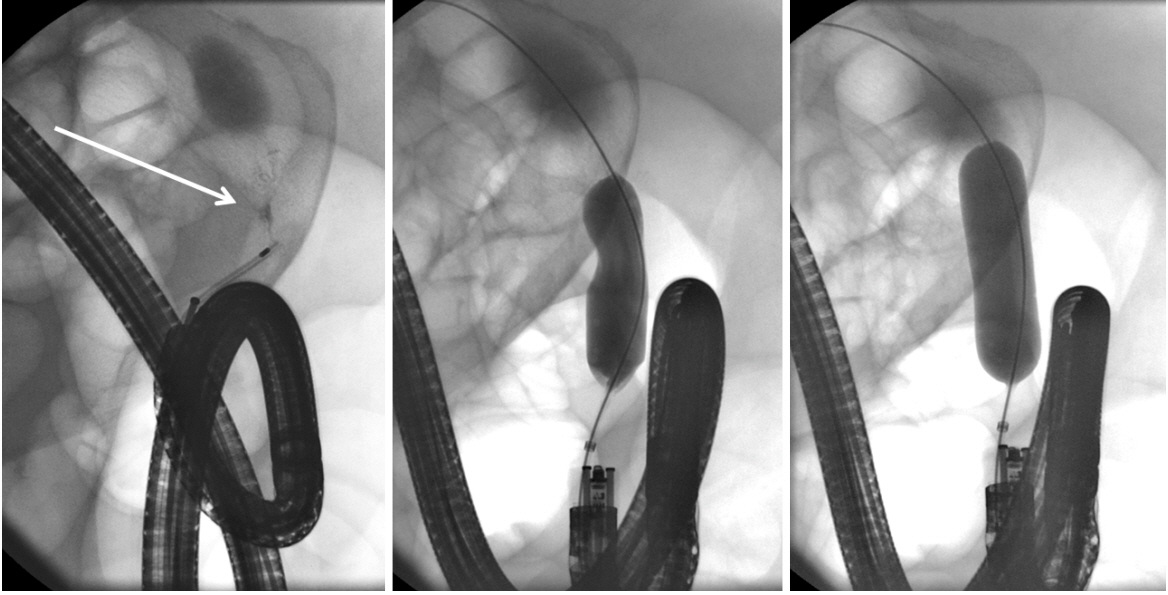
Fig. 2. A segment of short stenosis is delineated using injection of contrast via a catheter (arrow). Note the endoscope is in a torqued position secondary to postoperative adhesions. A balloon is advanced over a wire and carefully inflated until the indentation subsides.
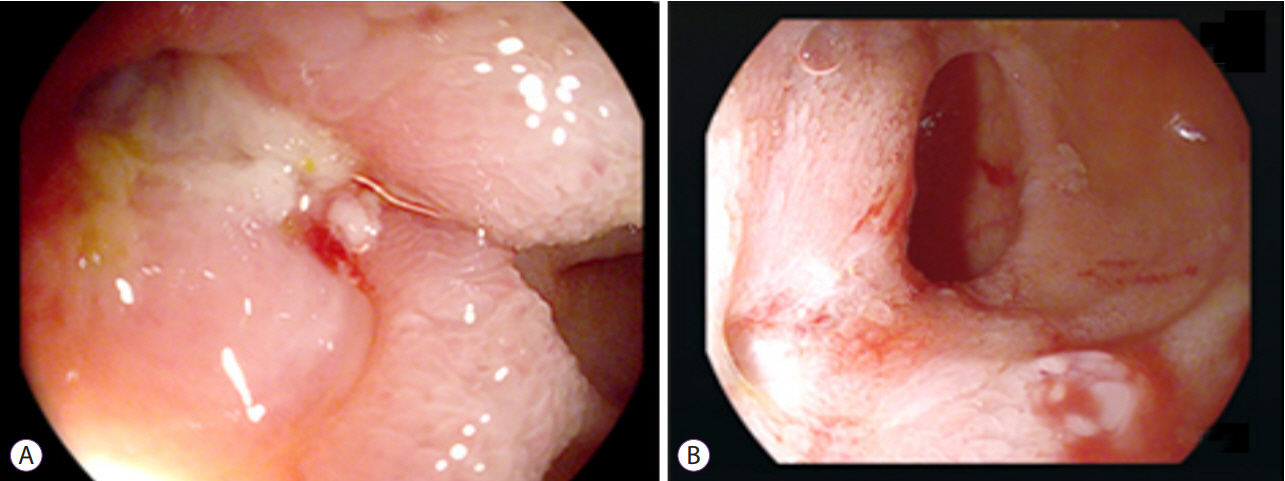
Fig. 3. (A) A suppurative fistula observed at the site of stenosis necessitated medical therapy and balloon dilatation. (B) Four months after dilation, discharge from the fistula is observed to have subsided.

Fig. 4. A site of jejunal stenosis is accessed using single-balloon endoscopy. (A) A guide wire is inserted across the stenosis. (B) A wire-guided balloon is positioned within the stenosis. (C) Water (or contrast)-filled balloons allow direct visual control during dilatation. (D) The stenosis is sufficiently dilated. A second narrowing, which was subsequently dilated is visible distal to the stenosis.
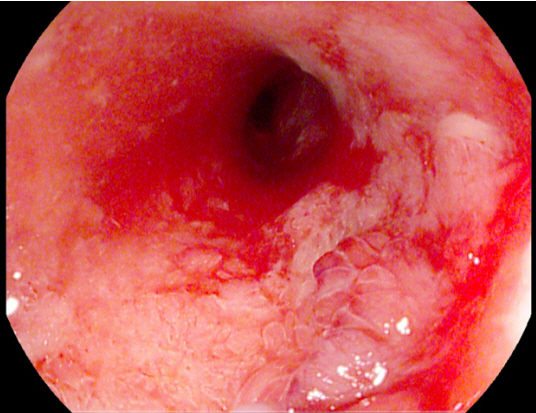
Fig. 5. Histologically confirmed low-grade intestinal neoplasia is observed at the site of a Crohn’s disease-associated stenosis (noted at the 4–5 o’clock position).
Cited by 2 articles
-
Update of endoscopic management of Crohn’s disease strictures
Akshay Pokala, Bo Shen
Intest Res. 2020;18(1):1-10. doi: 10.5217/ir.2019.09158.Endoscopic balloon dilations for strictures of rectum, ileocecal valve and duodenum in a patient with X-linked inhibitor of apoptosis deficiency: a case report
Shinsuke Otagiri, Takehiko Katsurada, Kensuke Sakurai, Junichi Sugita, Naoya Sakamoto
Intest Res. 2022;20(2):274-277. doi: 10.5217/ir.2021.00029.
Reference
-
1. Wehkamp J, Götz M, Herrlinger K, Steurer W, Stange EF. Inflammatory bowel disease. Dtsch Arztebl Int. 2016; 113:72–82.2. Cosnes J, Cattan S, Blain A, et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002; 8:244–250.
Article3. Bharadwaj S, Fleshner P, Shen B. Therapeutic armamentarium for stricturing Crohn’s disease: medical versus endoscopic versus surgical approaches. Inflamm Bowel Dis. 2015; 21:2194–2213.4. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990; 99:956–963.
Article5. Rueda Guzmán A, Wehkamp J, Kirschniak A, Naumann A, Malek NP, Goetz M. Endoscopic balloon dilatation of Crohn’s-associated intestinal strictures: high patient satisfaction and long-term efficacy. United European Gastroenterol J. 2016; 4:794–799.
Article6. Hirai F. Current status of endoscopic balloon dilation for Crohn’s disease. Intest Res. 2017; 15:166–173.
Article7. Navaneethan U, Lourdusamy V, Njei B, Shen B. Endoscopic balloon dilation in the management of strictures in Crohn’s disease: a systematic review and meta-analysis of non-randomized trials. Surg Endosc. 2016; 30:5434–5443.
Article8. Mueller T, Rieder B, Bechtner G, Pfeiffer A. The response of Crohn’s strictures to endoscopic balloon dilation. Aliment Pharmacol Ther. 2010; 31:634–639.
Article9. Van Assche G, Vermeire S, Rutgeerts P. Endoscopic therapy of strictures in Crohn’s disease. Inflamm Bowel Dis. 2007; 13:356–358. discussion 362-363.
Article10. Koltun WA. Dangers associated with endoscopic management of strictures in IBD. Inflamm Bowel Dis. 2007; 13:359–361. discussion 362-363.
Article11. Bettenworth D, Lopez R, Hindryckx P, Levesque BG, Rieder F. Heterogeneity in endoscopic treatment of Crohn’s disease-associated strictures: an international inflammatory bowel disease specialist survey. J Gastroenterol. 2016; 51:939–948.
Article12. Chen M, Shen B. Endoscopic therapy in Crohn’s disease: principle, preparation, and technique. Inflamm Bowel Dis. 2015; 21:2222–2240.13. Rieder F, Latella G, Magro F, et al. European Crohn’s and colitis organisation topical review on prediction, diagnosis and management of fibrostenosing Crohn’s disease. J Crohns Colitis. 2016; 10:873–885.
Article14. Dillman JR, Smith EA, Sanchez R, et al. Prospective cohort study of ultrasound-ultrasound and ultrasound-MR enterography agreement in the evaluation of pediatric small bowel Crohn disease. Pediatr Radiol. 2016; 46:490–497.
Article15. Ripollés T, Rausell N, Paredes JM, Grau E, Martínez MJ, Vizuete J. Effectiveness of contrast-enhanced ultrasound for characterisation of intestinal inflammation in Crohn’s disease: a comparison with surgical histopathology analysis. J Crohns Colitis. 2013; 7:120–128.
Article16. ASGE Standards of Practice Committee, Anderson MA, Ben-Menachem T, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointest Endosc. 2009; 70:1060–1070.
Article17. Veitch AM. Endoscopy in patients on antiplatelet agents and anticoagulants. Curr Treat Options Gastroenterol. 2017; 15:256–267.
Article18. Gustavsson A, Magnuson A, Blomberg B, Andersson M, Halfvarson J, Tysk C. Endoscopic dilation is an efficacious and safe treatment of intestinal strictures in Crohn’s disease. Aliment Pharmacol Ther. 2012; 36:151–158.
Article19. Hirai F, Matsui T, Yao K, Sou S, Seki T. Efficacy of carbon dioxide insufflation in endoscopic balloon dilation therapy by using double balloon endoscopy. Gastrointest Endosc. 2007; 66(3 Suppl):S26–S29.
Article20. Morar PS, Faiz O, Warusavitarne J, et al. Systematic review with meta-analysis: endoscopic balloon dilatation for Crohn’s disease strictures. Aliment Pharmacol Ther. 2015; 42:1137–1148.
Article21. Hassan C, Zullo A, De Francesco V, et al. Systematic review: endoscopic dilatation in Crohn’s disease. Aliment Pharmacol Ther. 2007; 26:1457–1464.
Article22. Gustavsson A, Magnuson A, Blomberg B, Andersson M, Halfvarson J, Tysk C. Smoking is a risk factor for recurrence of intestinal stricture after endoscopic dilation in Crohn’s disease. Aliment Pharmacol Ther. 2013; 37:430–437.
Article23. Oberhuber G, Stangl PC, Vogelsang H, Schober E, Herbst F, Gasche C. Significant association of strictures and internal fistula formation in Crohn’s disease. Virchows Arch. 2000; 437:293–297.
Article24. Fukumoto A, Tanaka S, Yamamoto H, et al. Diagnosis and treatment of small-bowel stricture by double balloon endoscopy. Gastrointest Endosc. 2007; 66(3 Suppl):S108–S112.
Article25. Greener T, Shapiro R, Klang E, et al. Clinical outcomes of surgery versus endoscopic balloon dilation for stricturing Crohn’s disease. Dis Colon Rectum. 2015; 58:1151–1157.
Article26. Lian L, Stocchi L, Remzi FH, Shen B. Comparison of endoscopic dilation vs surgery for anastomotic stricture in patients with Crohn’s disease following ileocolonic resection. Clin Gastroenterol Hepatol. 2017; 15:1226–1231.27. Nepal S, Bahuva R, Shen B, Atreja A. Early initiation of biologics and immunomodulators decrease the need for surgery in enterography proven stricturing Crohn’s disease. Gastroenterology. 2012; 142(5 Suppl 1):S64–S65.28. Lawrance IC, Welman CJ, Shipman P, Murray K. Correlation of MRI-determined small bowel Crohn’s disease categories with medical response and surgical pathology. World J Gastroenterol. 2009; 15:3367–3375.
Article29. Bouguen G, Trouilloud I, Siproudhis L, et al. Long-term outcome of non-fistulizing (ulcers, stricture) perianal Crohn’s disease in patients treated with infliximab. Aliment Pharmacol Ther. 2009; 30:749–756.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current status of endoscopic balloon dilation for Crohn's disease
- Use of a Cutting Balloon Dilation as a Rescue Therapy in Patients with Benign Bilioenteric Anastomotic Strictures Refractory to Conventional Balloon Dilation
- Update of endoscopic management of Crohn’s disease strictures
- The Role of Endoscopic Balloon Dilation in the Treatment of Esophageal Strictures
- Difficulty of balloon dilatation in corrosive esophageal strictures
