Shear-Wave Elastography of the Breast: Added Value of a Quality Map in Diagnosis and Prediction of the Biological Characteristics of Breast Cancer
- Affiliations
-
- 1Department of Ultrasound, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China. zhoujh@sysucc.org.cn
- 2Department of Anesthesiology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
- KMID: 2471634
- DOI: http://doi.org/10.3348/kjr.2019.0453
Abstract
OBJECTIVE
To determine the added value of a shear-wave elastography (SWE) quality map (QM) in the diagnosis of breast lesions and in predicting the biological characteristics of invasive breast cancer.
MATERIALS AND METHODS
Between January 2016 and February 2019, this study included 368 women with 368 pathologically proven breast lesions, which appeared as poor-quality regions in the QM of SWE. To measure shear-wave velocity (SWV), seven regions of interest were placed in each lesion with and without QM guidance. Under QM guidance, poor-quality areas were avoided. Diagnostic performance was calculated for mean SWV (SWV(mean)), max SWV (SWV(max)), and standard deviation (SD) with QM guidance (SWV(mean) + QM, SWV(max) + QM, and SD + QM, respectively) and without QM guidance (SWV(mean) − QM, SWV(max) − QM, and SD − QM, respectively). For invasive cancers, the relationship between SWV findings and biological characteristics was investigated with and without QM guidance.
RESULTS
Of the 368 women (mean age, 47 years; SD, 10.8 years) enrolled, 159 had benign breast lesions and 209 had malignant breast lesions. SWV(mean) + QM (3.6 ± 1.39 m/s) and SD + QM (1.02 ± 0.84) were significantly different from SWV(mean) − QM (3.29 ± 1.22 m/s) and SD − QM (1.46 ± 1.06), respectively (all p < 0.001). For differential diagnosis of breast lesions, the sensitivity and areas under the receiver operating characteristic curve (AUC) of SWV(mean) + QM (sensitivity: 89%; AUC: 0.932) were better than those of SWV(mean) − QM (sensitivity, 84.2%; AUC, 0.912) (all p < 0.05). There was no significant difference in sensitivity and specificity between SD + QM and SD − QM (all p = 1.000). Among the biological characteristics of invasive cancers, lymphovascular involvement, axillary lymph node metastasis, negative estrogen receptor status, negative progesterone receptor status, positive human epidermal growth factor receptor status, and aggressive molecular subtypes showed higher SWV(mean) + QM (all p < 0.05), while only lymphovascular involvement showed higher SWV(mean) − QM (p = 0.036).
CONCLUSION
The use of QM in SWE might improve the diagnostic performance for breast lesions and facilitate prediction of the biological characteristics of invasive breast cancers.
Keyword
MeSH Terms
-
Area Under Curve
Breast Neoplasms*
Breast*
Diagnosis*
Diagnosis, Differential
Elasticity Imaging Techniques*
Estrogens
Female
Humans
Lymph Nodes
Neoplasm Metastasis
Population Characteristics*
Receptor, Epidermal Growth Factor
Receptors, Progesterone
ROC Curve
Sensitivity and Specificity
Ultrasonography
Estrogens
Receptor, Epidermal Growth Factor
Receptors, Progesterone
Figure
-
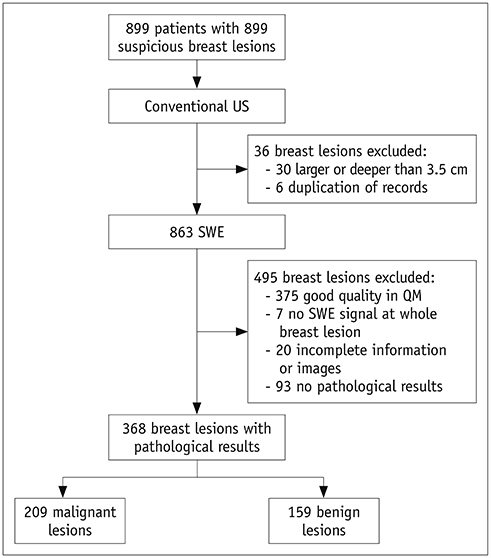
Fig. 1 Study flow diagram. QM = quality map, SWE = shear-wave elastography, US = ultrasound
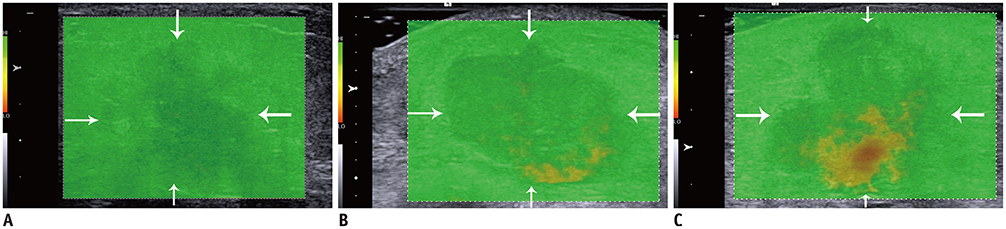
Fig. 2 Quality evaluation standard of QM. A. Breast lesion (arrows) is displayed as evenly green in QM, which indicates good quality. B. Quality of this breast lesion (arrows) is considered as poor, and yellow components in QM should be avoided while measuring SWV. C. Quality of this breast lesion (arrows) is considered to be poor, and red and yellow components in QM should be avoided while measuring SWV. SWV = shear-wave velocity
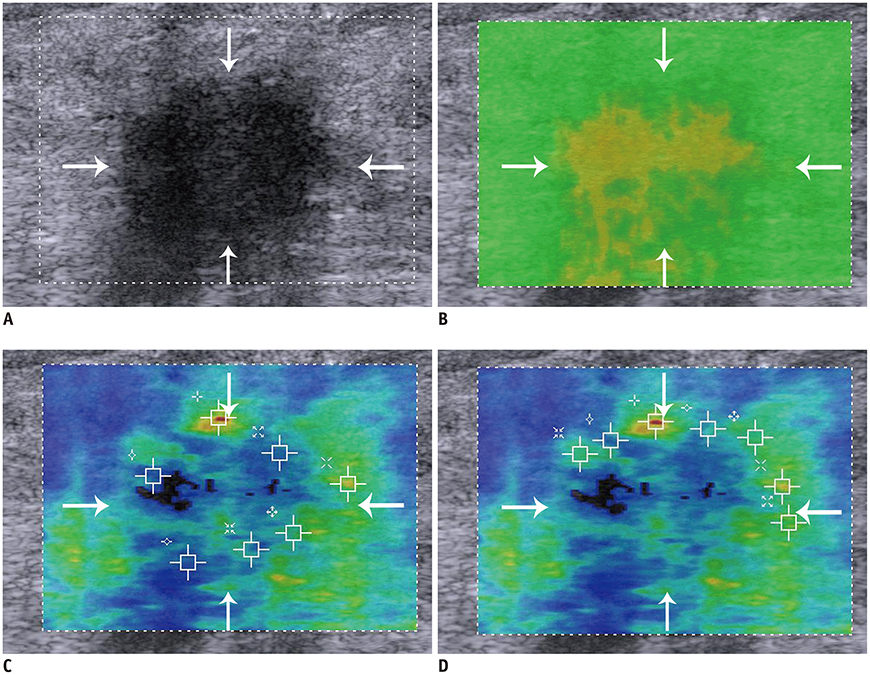
Fig. 3 Invasive ductal carcinoma in 53-year-old woman. A. Lesion (arrows) is classified as Breast Imaging Reporting and Data System 4C on B-mode US. B. Lesion (arrows) shows poor quality in QM of SWE. C. Mean SWV without QM guidance (SWVmean − QM) of breast lesion (arrows) is 2.97 m/s, misdiagnosing this lesion as benign. D. Mean SWV with QM guidance (SWVmean + QM) of breast lesion (arrows) is 3.17 m/s, assessing this lesion as malignant.
Reference
-
1. Shiina T, Nightingale KR, Palmeri ML, Hall TJ, Bamber JC, Barr RG, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 1: basic principles and terminology. Ultrasound Med Biol. 2015; 41:1126–1147.
Article2. Barr RG, Nakashima K, Amy D, Cosgrove D, Farrokh A, Schafer F, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 2: breast. Ultrasound Med Biol. 2015; 41:1148–1160.
Article3. Cho N, Jang M, Lyou CY, Park JS, Choi HY, Moon WK. Distinguishing benign from malignant masses at breast US: combined US elastography and color doppler US--influence on radiologist accuracy. Radiology. 2012; 262:80–90.
Article4. Berg WA, Cosgrove DO, Doré CJ, Schäfer FK, Svensson WE, Hooley RJ, et al. BE1 Investigators. Shear-wave elastography improves the specificity of breast US: the BE1 multinational study of 939 masses. Radiology. 2012; 262:435–449.
Article5. Li DD, Xu HX, Guo LH, Bo XW, Li XL, Wu R, et al. Combination of two-dimensional shear wave elastography with ultrasound breast imaging reporting and data system in the diagnosis of breast lesions: a new method to increase the diagnostic performance. Eur Radiol. 2016; 26:3290–3300.
Article6. Lee EJ, Jung HK, Ko KH, Lee JT, Yoon JH. Diagnostic performances of shear wave elastography: which parameter to use in differential diagnosis of solid breast masses? Eur Radiol. 2013; 23:1803–1811.
Article7. Gweon HM, Youk JH, Son EJ, Kim JA. Visually assessed colour overlay features in shear-wave elastography for breast masses: quantification and diagnostic performance. Eur Radiol. 2013; 23:658–663.
Article8. Evans A, Whelehan P, Thomson K, McLean D, Brauer K, Purdie C, et al. Invasive breast cancer: relationship between shear-wave elastographic findings and histologic prognostic factors. Radiology. 2012; 263:673–677.
Article9. Chang JM, Park IA, Lee SH, Kim WH, Bae MS, Koo HR, et al. Stiffness of tumours measured by shear-wave elastography correlated with subtypes of breast cancer. Eur Radiol. 2013; 23:2450–2458.
Article10. Youk JH, Gweon HM, Son EJ, Kim JA, Jeong J. Shear-wave elastography of invasive breast cancer: correlation between quantitative mean elasticity value and immunohistochemical profile. Breast Cancer Res Treat. 2013; 138:119–126.
Article11. Bai M, Du L, Gu J, Li F, Jia X. Virtual touch tissue quantification using acoustic radiation force impulse technology: initial clinical experience with solid breast masses. J Ultrasound Med. 2012; 31:289–294.12. Barr RG. Shear wave imaging of the breast: still on the learning curve. J Ultrasound Med. 2012; 31:347–350.13. Barr RG, Zhang Z. Shear-wave elastography of the breast: value of a quality measure and comparison with strain elastography. Radiology. 2015; 275:45–53.
Article14. Zheng X, Huang Y, Wang Y, Liu Y, Li F, Han J, et al. Combination of different types of elastography in downgrading ultrasound breast imaging-reporting and data system category 4a breast lesions. Breast Cancer Res Treat. 2019; 174:423–432.
Article15. Harbeck N, Gnant M. Breast cancer. Lancet. 2017; 389:1134–1150.
Article16. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44:837–845.
Article17. Youk JH, Gweon HM, Son EJ. Shear-wave elastography in breast ultrasonography: the state of the art. Ultrasonography. 2017; 36:300–309.
Article18. Barr RG. Sonographic breast elastography: a primer. J Ultrasound Med. 2012; 31:773–783.19. Li XL, Xu HX, Bo XW, Liu BJ, Huang X, Li DD, et al. Value of virtual touch tissue imaging quantification for evaluation of ultrasound breast imaging-reporting and data system category 4 lesions. Ultrasound Med Biol. 2016; 42:2050–2057.
Article20. Ianculescu V, Ciolovan LM, Dunant A, Vielh P, Mazouni C, Delaloge S, et al. Added value of Virtual Touch IQ shear wave elastography in the ultrasound assessment of breast lesions. Eur J Radiol. 2014; 83:773–777.
Article21. Barr RG, Zhang Z. Effects of precompression on elasticity imaging of the breast: development of a clinically useful semiquantitative method of precompression assessment. J Ultrasound Med. 2012; 31:895–902.22. Cosgrove DO, Berg WA, Doré CJ, Skyba DM, Henry JP, Gay J, et al. Shear wave elastography for breast masses is highly reproducible. Eur Radiol. 2012; 22:1023–1032.
Article23. Ferraioli G, Tinelli C, Dal Bello B, Zicchetti M, Filice G, Filice C. Liver Fibrosis Study Group. Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C: a pilot study. Hepatology. 2012; 56:2125–2133.
Article24. Baker EL, Lu J, Yu D, Bonnecaze RT, Zaman MH. Cancer cell stiffness: integrated roles of three-dimensional matrix stiffness and transforming potential. Biophys J. 2010; 99:2048–2057.
Article25. Youk JH, Kim EK, Kim MJ, Kwak JY, Son EJ. Analysis of false-negative results after US-guided 14-gauge core needle breast biopsy. Eur Radiol. 2010; 20:782–789.
Article26. Crystal P, Koretz M, Shcharynsky S, Makarov V, Strano S. Accuracy of sonographically guided 14-gauge core-needle biopsy: results of 715 consecutive breast biopsies with at least two-year follow-up of benign lesions. J Clin Ultrasound. 2005; 33:47–52.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Future of breast elastography
- Shear-wave elastography in breast ultrasonography: the state of the art
- Diagnostic Performance of Quantitative Shear Wave Ultrasound Elastography for Thyroid Cancer
- Elastography of the Breast: Imaging Techniques and Pitfalls in Interpretation
- Ductal Carcinoma In Situ Detected by Shear Wave Elastography within a Fibroadenoma
