Pharmacological and Mechanical Thromboprophylaxis in Critically Ill Patients: a Network Meta-Analysis of 12 Trials
- Affiliations
-
- 1Department of Internal Medicine and Cardiovascular Center, Seoul National University Hospital, Seoul, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Korea.
- 3Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 4Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. lungdrcho@gmail.com
- KMID: 2470282
- DOI: http://doi.org/10.3346/jkms.2016.31.11.1828
Abstract
- Thromboprophylaxis for venous thromboembolism is widely used in critically ill patients. However, only limited evidence exists regarding the efficacy and safety of the various thromboprophylaxis techniques, especially mechanical thromboprophylaxis. Therefore, we performed meta-analysis of randomized controlled trials (RCTs) that compared the overall incidence of deep vein thrombosis (DVT) for between unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and intermittent pneumatic compression (IPC) in critically ill patients. A Bayesian random effects model for multiple treatment comparisons was constructed. The primary outcome measure was the overall incidence of DVT at the longest follow-up. The secondary outcome measure was the incidence of major bleeding, as defined by the original trials. Our analysis included 8,622 patients from 12 RCTs. The incidence of DVT was significantly lower in patients treated with UFH (OR, 0.45; 95% CrI, 0.22-0.83) or LMWH (OR, 0.38; 95% CrI, 0.18-0.72) than in patients in the control group. IPC was associated with a reduced incidence of DVT compared to the control group, but the effect was not statistically significant (OR, 0.50; 95% CrI, 0.20-1.23). The risk of DVT was similar for patients treated with UFH and LMWH (OR, 1.16; 95% CrI, 0.68-2.11). The risk of major bleeding was similar between the treatment groups in medical critically ill patients and also in critically ill patients with a high risk of bleeding. In critically ill patients, the efficacy of mechanical thromboprophylaxis in reducing the risk of DVT is not as robust as those of pharmacological thromboprophylaxis.
MeSH Terms
-
Anticoagulants/*therapeutic use
Bayes Theorem
Critical Illness
Databases, Factual
Heparin/*therapeutic use
Heparin, Low-Molecular-Weight/*therapeutic use
Humans
Incidence
Intermittent Pneumatic Compression Devices
Odds Ratio
Venous Thromboembolism/*prevention & control
Venous Thrombosis/epidemiology/etiology
Anticoagulants
Heparin, Low-Molecular-Weight
Heparin
Figure
-
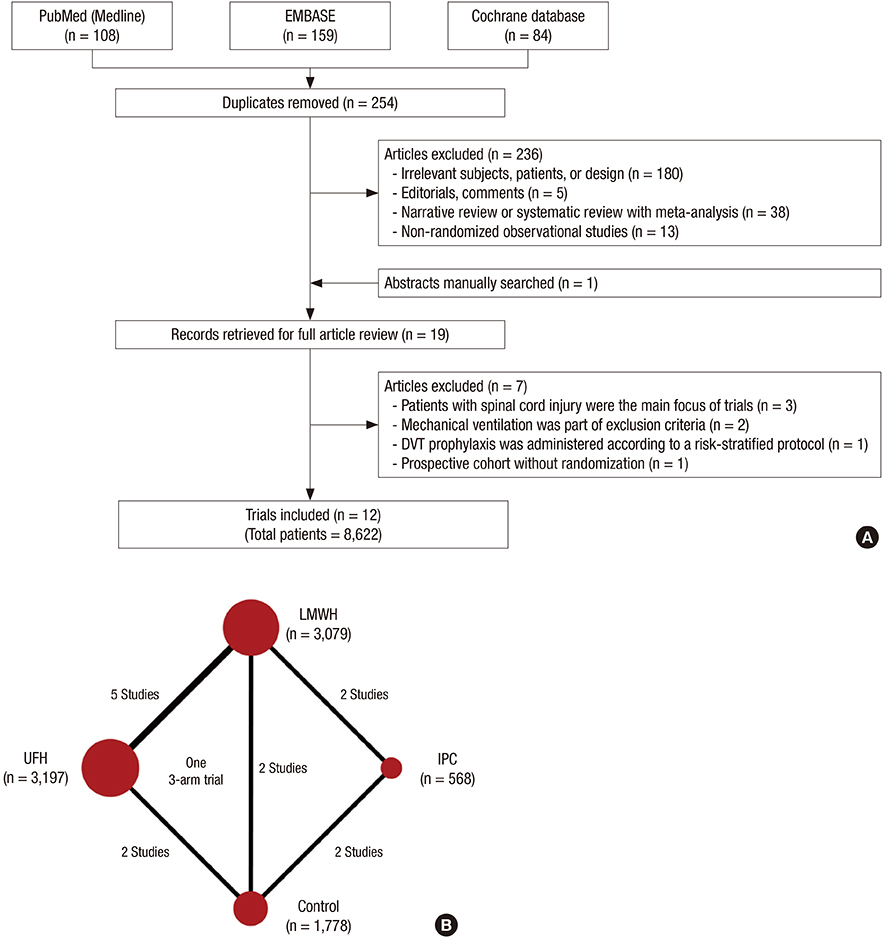
Fig. 1 Flow diagram of trial selection and network plot of the meta-analysis. (A) The flow diagram follows the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). (B) Network plot of meta-analysis model: each treatment is represented by a node; the size of the node is proportional to the sample size randomized to each group and the thickness of the line connecting the nodes is proportional to the total randomized sample size in each pair-wise comparison. LMWH = low-molecular-weight heparin, IPC = intermittent pneumatic compression, UFH = unfractionated heparin.
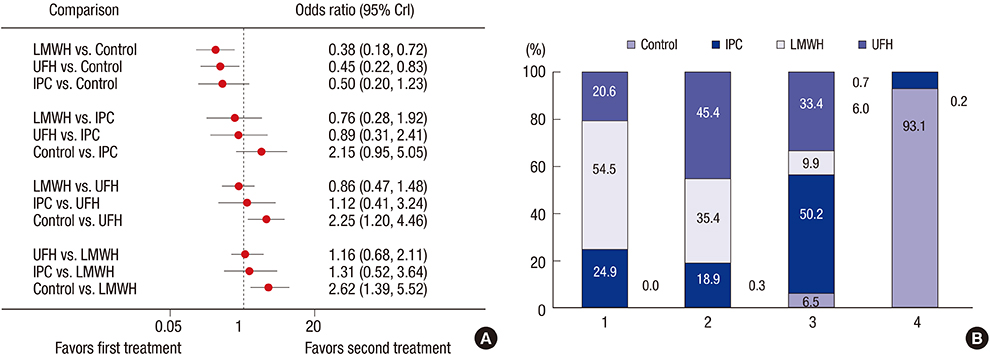
Fig. 2 Comparative efficacy of thromboprophylaxis interventions in the prevention of deep vein thrombosis (DVT). (A) Estimated odds ratios (ORs) and 95% credible intervals (CrIs) for DVT from network meta-analysis for different thromboprophylaxis interventions, according to a Bayesian network meta-analysis with random effects model. The circles and horizontal lines indicate pair-wise OR and 95% CrI, respectively. (B) Rank probability of each treatment arm for the risk of DVT. The number on the horizontal axis is the possible rank of each treatment, from best to worst according to the outcome. The size of each bar corresponds to the probability of each treatment being at a specific rank. LMWH = low-molecular-weight heparin, IPC = intermittent pneumatic compression, UFH = unfractionated heparin.
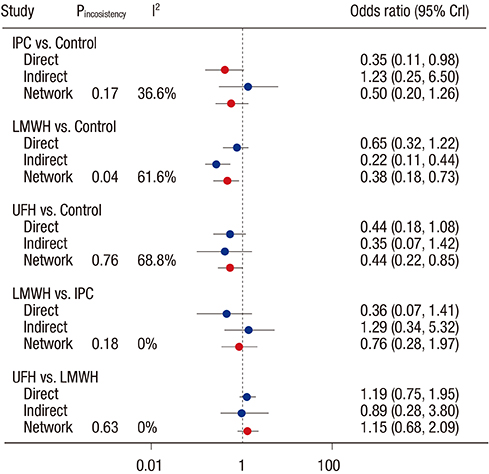
Fig. 3 Analysis of consistency and heterogeneity in the network meta-analysis model for the risk of deep vein thrombosis. LMWH = low-molecular-weight heparin, IPC = intermittent pneumatic compression, UFH = unfractionated heparin.
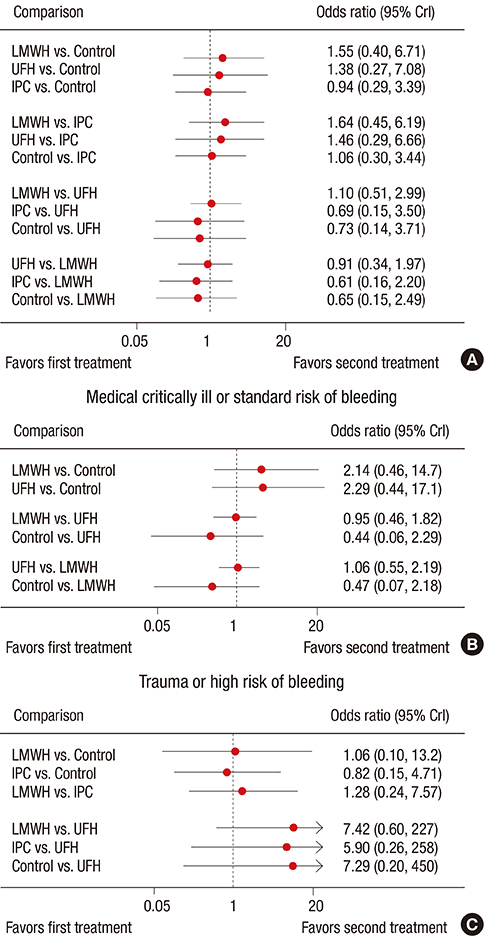
Fig. 4 Comparative safety of thromboprophylaxis interventions for the risk of major bleeding. (A) Estimated odds ratios (ORs) and 95% credible intervals (CrIs) for major bleeding from eight trials reporting the incidence of major bleeding. (B) Estimated OR and 95% CrI for major bleeding from four trials that included medical critically ill patients with a standard risk of bleeding. (C) Estimated OR and 95% CrI for major bleeding from four trials that included surgical or trauma critically ill patients with a high risk of bleeding. The circles and horizontal lines indicate Bayesian ORs and 95% CrIs, respectively.
Reference
-
1. Moser KM, LeMoine JR, Nachtwey FJ, Spragg RG. Deep venous thrombosis and pulmonary embolism. Frequency in a respiratory intensive care unit. JAMA. 1981; 246:1422–1424.2. Geerts W, Cook D, Selby R, Etchells E. Venous thromboembolism and its prevention in critical care. J Crit Care. 2002; 17:95–104.3. Cook DJ, Donadini MP. Pulmonary embolism in medical-surgical critically ill patients. [vii.]. Hematol Oncol Clin North Am. 2010; 24:677–682.4. Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, Cook DJ, Balekian AA, Klein RC, Le H, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012; 141:e195S–e226S.5. Alhazzani W, Lim W, Jaeschke RZ, Murad MH, Cade J, Cook DJ. Heparin thromboprophylaxis in medical-surgical critically ill patients: a systematic review and meta-analysis of randomized trials. Crit Care Med. 2013; 41:2088–2098.6. Kakkos SK, Caprini JA, Geroulakos G, Nicolaides AN, Stansby GP, Reddy DJ. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. 2008; CD005258.7. Silbersack Y, Taute BM, Hein W, Podhaisky H. Prevention of deep-vein thrombosis after total hip and knee replacement. Low-molecular-weight heparin in combination with intermittent pneumatic compression. J Bone Joint Surg Br. 2004; 86:809–812.8. Eisele R, Kinzl L, Koelsch T. Rapid-inflation intermittent pneumatic compression for prevention of deep venous thrombosis. J Bone Joint Surg Am. 2007; 89:1050–1056.9. Lauzier F, Turgeon AF, Boutin A, Shemilt M, Côté I, Lachance O, Archambault PM, Lamontagne F, Moore L, Bernard F, et al. Clinical outcomes, predictors, and prevalence of anterior pituitary disorders following traumatic brain injury: a systematic review. Crit Care Med. 2014; 42:712–721.10. Zhang C, Zeng W, Zhou H, Zheng BX, Cheng JC, Li XY, Jiang YP, Jiang LD, Li XJ. The efficacy of intermittent pneumatic compression in the prevention of venous thromboembolism in medical critically ill patients. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2011; 23:563–565.11. Vignon P, Dequin PF, Renault A, Mathonnet A, Paleiron N, Imbert A, Chatellier D, Gissot V, Lhéritier G, Aboyans V, et al. Intermittent pneumatic compression to prevent venous thromboembolism in patients with high risk of bleeding hospitalized in intensive care units: the CIREA1 randomized trial. Intensive Care Med. 2013; 39:872–880.12. Egger M, Zellweger-Zähner T, Schneider M, Junker C, Lengeler C, Antes G. Language bias in randomised controlled trials published in English and German. Lancet. 1997; 350:326–329.13. Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0 [Internet]. updated March 2011. accessed on 4 September 2016. Available at http://handbook.cochrane.org.14. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996; 17:1–12.15. Lumley T. Network meta-analysis for indirect treatment comparisons. Stat Med. 2002; 21:2313–2324.16. Gelman A, Rubin DB. Inference from iterative simulation using multiple sequences. Stat Sci. 1992; 7:457–472.17. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009; 151:264–269. W6418. Geerts WH, Jay RM, Code KI, Chen E, Szalai JP, Saibil EA, Hamilton PA. A comparison of low-dose heparin with low-molecular-weight heparin as prophylaxis against venous thromboembolism after major trauma. N Engl J Med. 1996; 335:701–707.19. Cook D, Meade M, Guyatt G, Walter S, Heels-Ansdell D, Warkentin TE, Zytaruk N, Crowther M, Geerts W, Cooper DJ, et al. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med. 2011; 364:1305–1314.20. Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med. 1982; 10:448–450.21. Goldhaber SZ, Kett DH, Cusumano CJ, Kuroki CA. Low molecular weight heparin versus minidose unfractionated heparin for prophylaxis against venous thromboembolism in medical intensive care unit patients: a randomized controlled trial. J Am Coll Cardiol. 2000; 35:A325.22. De A, Roy P, Garg VK, Pandey NK. Low-molecular-weight heparin and unfractionated heparin in prophylaxis against deep vein thrombosis in critically ill patients undergoing major surgery. Blood Coagul Fibrinolysis. 2010; 21:57–61.23. Fraisse F, Holzapfel L, Couland JM, Simonneau G, Bedock B, Feissel M, Herbecq P, Pordes R, Poussel JF, Roux L, et al. Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD. Am J Respir Crit Care Med. 2000; 161:1109–1114.24. Ginzburg E, Cohn SM, Lopez J, Jackowski J, Brown M, Hameed SM; Miami Deep Vein Thrombosis Study Group. Randomized clinical trial of intermittent pneumatic compression and low molecular weight heparin in trauma. Br J Surg. 2003; 90:1338–1344.25. Kapoor M, Kupfer YY, Tessler S. Subcutaneous heparin prophylaxis significantly reduces the incidence of venous thromboembolic events in the critically ill. Crit Care Med. 1999; 27:A69.26. Shorr AF, Williams MD. Venous thromboembolism in critically ill patients. Observations from a randomized trial in sepsis. Thromb Haemost. 2009; 101:139–144.27. Kurtoglu M, Yanar H, Bilsel Y, Guloglu R, Kizilirmak S, Buyukkurt D, Granit V. Venous thromboembolism prophylaxis after head and spinal trauma: intermittent pneumatic compression devices versus low molecular weight heparin. World J Surg. 2004; 28:807–811.28. Limpus A, Chaboyer W, McDonald E, Thalib L. Mechanical thromboprophylaxis in critically ill patients: a systematic review and meta-analysis. Am J Crit Care. 2006; 15:402–410.29. Lamontagne F, McIntyre L, Dodek P, Heels-Ansdell D, Meade M, Pemberton J, Skrobik Y, Seppelt I, Vlahakis NE, Muscedere J, et al. Nonleg venous thrombosis in critically ill adults: a nested prospective cohort study. JAMA Intern Med. 2014; 174:689–696.30. Lachmann EA, Rook JL, Tunkel R, Nagler W. Complications associated with intermittent pneumatic compression. Arch Phys Med Rehabil. 1992; 73:482–485.31. Won SH, Lee YK, Suh YS, Koo KH. Extensive bullous complication associated with intermittent pneumatic compression. Yonsei Med J. 2013; 54:801–802.32. Siddiqui AU, Buchman TG, Hotchkiss RS. Pulmonary embolism as a consequence of applying sequential compression device on legs in a patient asymptomatic of deep vein thrombosis. Anesthesiology. 2000; 92:880–882.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of a Clinical Nursing Practice Guideline of Enteral Nutrition Care on the Duration of Mechanical Ventilator for Critically Ill Patients
- When and why to start continuous renal replacement therapy in critically ill patients with acute kidney injury
- Glycemic control in acute illness
- Meta-epidemiology
- Pharmacological strategies to prevent postoperative delirium: a systematic review and network meta-analysis
