Focal Xanthogranulomatous Pyelonephritis Associated with Xanthogranulomatous Cholecystitis: A Case Report
- Affiliations
-
- 1Department of Radiology, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. kyhkim@hanmail.net
- 2Department of Pathology, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 3Department of General Surgery, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- KMID: 2469192
- DOI: http://doi.org/10.3348/jksr.2020.81.1.190
Abstract
- Xanthogranulomatous inflammation is a rare inflammatory reaction, characterized by lipid-laden macrophages, known as xanthomas, in histopathologic examination. Aggressive xanthogranulomatous inflammation often manifests as local infiltration but does not affect distant organs unless combined with rare systemic diseases. We report a case of focal xanthogranulomatous pyelonephritis (XGP) associated with severe xanthogranulomatous cholecystitis. Focal XGP was suspected in radiologic examination that showed a cystic lesion with an infiltrative margin, which were surgically resected and confirmed in pathologic examination. To our knowledge, this is the first report of focal xanthogranulomatous pyelonephritis associated with xanthogranulomatous cholecystitis. Moreover, we found peripheral hypointensity around the cystic lesion in the T2-weighted image, probably reflecting hemorrhage and fibrosis of the xanthogranulomatous inflammation.
MeSH Terms
Figure
-
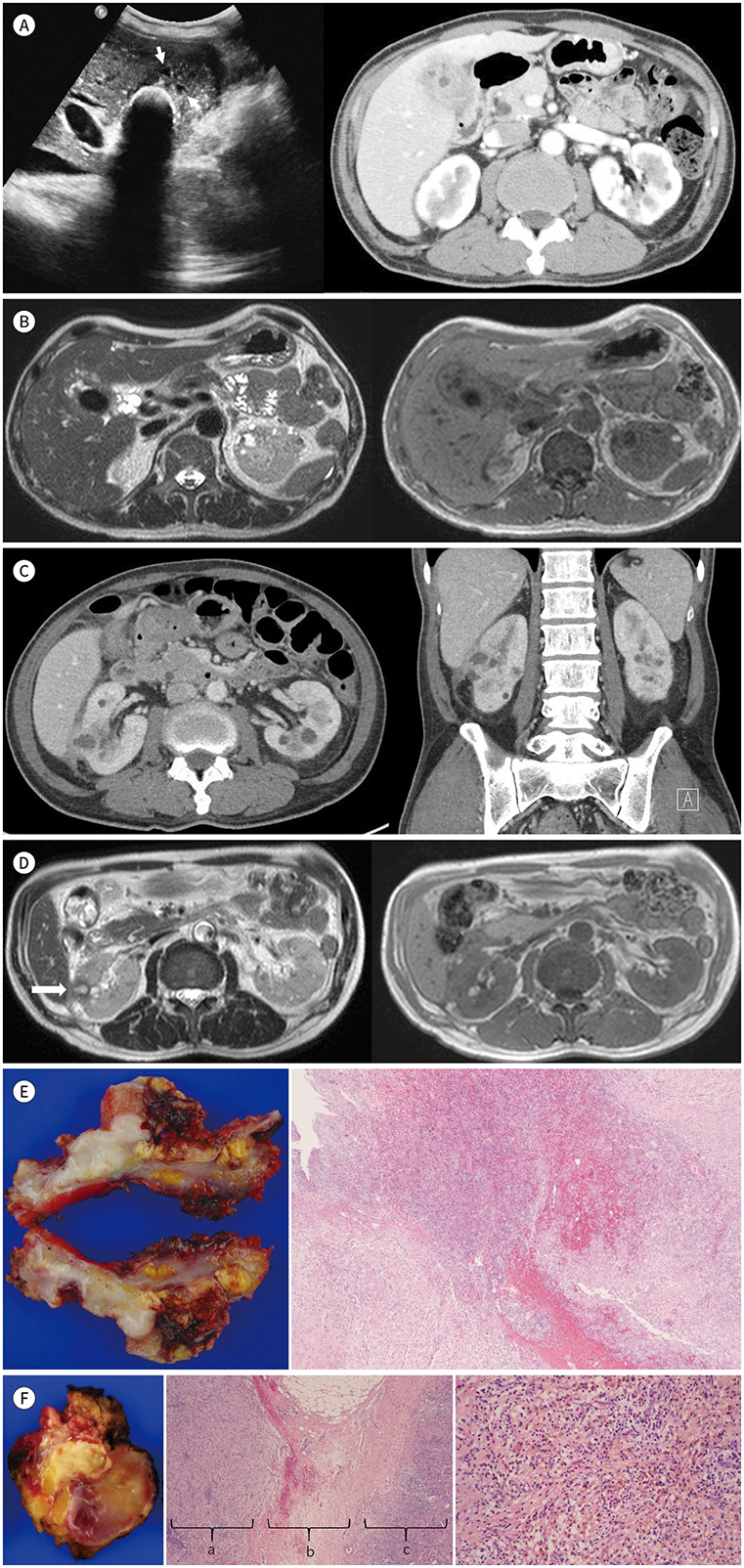
Fig. 1 Focal xanthogranulomatous pyelonephritis associated with xanthogranulomatous cholecystitis in a 56-year-old man, presenting with right upper quadrant pain. A. On ultrasonography (left panel), a GB stone is seen as a curvilinear hyper-reflective echo with distal acoustic shadowing. A few anechoic nodules (arrows) are noted within the thickened isoechoic GB walls. Axial CT (right panel) shows diffuse wall thickening of GB with intramural low-attenuation nodules. B. Axial T2- (left panel) and T1-weighted imaging (right panel) show oval GB stones as a dark signal and intramural nodules as a high signal. C. Axial CT shows a cystic lesion in the right kidney with infiltration extending peripherally to the perirenal tissues and hepatorenal recess. Coronal CT better illustrates the infiltrative lesion between the liver and the kidney with focal peritoneal wall thickening. D. Axial T2-weighted imaging (left panel) shows a nodular hyperintense lesion with rim-like low signal intensity (arrow). This lesion is not clearly outlined on the T1-weighted image (right panel). E. The gross specimen of GB shows disfigurement with marked irregular mural fibrous thickening, multifocal extensive mucosal ulcers, transmural old hemorrhages, and multiple yellowish xanthogranulomatous nodules or plaques (left panel). Scanning photomicrograph of GB wall exhibiting mucosal ulcers, transmural hemorrhages, dense mural fibrosis, and nodular aggregates of foamy histiocytes and inflammatory cells (right panel, × 40, H&E stain). F. The gross specimen of the right renal cortex and perirenal fibroadipose tissues (left panel) reveal a few prominent yellowish xanthogranulomatous nodules or plaques, fresh-to-old hemorrhages, and dense fibrous adhesion. Scanning photomicrography shows massive perirenal (a) and subcapsular (c) collection of foamy histiocytes, dense pericapsular fibrosis (b), and inflammatory cell infiltration (middle panel, × 40, H&E stain). Yellowish xanthogranulomatous nodules demonstrate abundant lipid-laden foamy histiocytes and hemosiderin-laden histiocytes, admixed with polymorphic lymphoreticular cells and fibroblasts (right panel, × 200, H&E stain). GB = gallbladder, H&E = hematoxylin and eosin
Reference
-
1. Bourm KS, Menias CO, Ali K, Alhalabi K, Elsayes KM. Spectrum of xanthogranulomatous processes in the abdomen and pelvis: a pictorial review of infectious, inflammatory, and proliferative responses. AJR Am J Roentgenol. 2017; 208:475–484.
Article2. Kuo CC, Wu CF, Huang CC, Lee YJ, Lin WC, Tsai CW, et al. Xanthogranulomatous pyelonephritis: critical analysis of 30 patients. Int Urol Nephrol. 2011; 43:15–22.
Article3. Kaushik R, Attri AK. Choleretroperitoneum-an unusual complication of cholelithiasis. Indian J Surg. 2004; 66:358–360.4. Roels K, Bogaert J, Van Hoe L, Vanbeckevoort D, Delvaux S. Xanthogranulomatous cholecystitis associated with a xanthogranulomatous pseudotumour on the left diaphragm. Eur Radiol. 1999; 9:1139–1141.
Article5. Losanoff JE, Reichman TW, Steinberg GD, Millis JM. Duodenal diverticulum causing xanthogranulomatous pyelonephritis with multiorgan involvement: first case report. Digestion. 2006; 74:236–237.
Article6. Verswijvel G, Oyen R, Van Poppel H, Roskams T. Xanthogranulomatous pyelonephritis: MRI findings in the diffuse and the focal type. Eur Radiol. 2000; 10:586–589.
Article7. Song YS, Lee IS, Choi KU, Cho KH, Lee SM, Lee YH, et al. Soft tissue masses showing low signal intensity on T2-weighted images: correlation with pathologic findings. J Korean Soc Magn Reson Med. 2014; 18:279–289.
Article8. Cakmakci H, Tasdelen N, Obuz F, Yilmaz E, Kovanlikaya A. Pediatric focal xanthogranulomatous pyelonephritis: dynamic contrast-enhanced MRI findings. Clin Imaging. 2002; 26:183–186.9. Chang BJ, Kim SH, Park HY, Lim SW, Kim J, Lee KH, et al. Distinguishing xanthogranulomatous cholecystitis from the wall-thickening type of early-stage gallbladder cancer. Gut Liver. 2010; 4:518–523.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Xanthogranulomatous Pyelonephritis
- A case of xanthogranulomatous pyelonephritis
- Two Cases of Xanthogranulomatous Pyelonephritis
- Xanthogranulomatous Pyelonephritis: A Case Report and Review of the Literature
- A Case of Xanthogranulomatous Pyelonephritis which was Confused with Renal Pelvic Tumor
