Functional Outcomes After Critical Pathway for Inpatient Rehabilitation of Total Knee Arthroplasty
- Affiliations
-
- 1Department of Rehabilitation Medicine, Jeju National University College of Medicine—Regional Rheumatoid and Degenerative Arthritis Center, Jeju National University Hospital, Jeju, Korea. brkim08@jejunu.ac.kr
- 2Department of Orthopedic Surgery, Jeju National University College of Medicine—Regional Rheumatoid and Degenerative Arthritis Center, Jeju National University Hospital, Jeju, Korea.
- KMID: 2468692
- DOI: http://doi.org/10.5535/arm.2019.43.6.650
Abstract
OBJECTIVE
To investigate functional outcomes after the application of a critical pathway for inpatient rehabilitation of total knee arthroplasty (TKA).
METHODS
A total of 184 patients (57 males and 127 females; average age, 71.5±5.9 years) who underwent unilateral or bilateral TKA were included. The critical pathway included early, intensive individualized rehabilitation exercises. Patients completed the following performance-based physical function tests: the stair climbing test (SCT), 6-minute walk test (6MWT), and Timed Up and Go test (TUG) as well as measurement of isometric knee flexor and extensor strength of the operated knee, gait speed, and range of knee flexion and extension. Self-reported physical function and pain were measured using the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) and visual analog scale (VAS), respectively, and self-reported quality of life was measured using the EuroQoL 5 dimension (EQ-5D) questionnaire. These evaluations were performed preoperatively and at 1 month and 3 months postoperatively.
RESULTS
Performance-based and self-reported physical function and quality of life measures improved nonlinearly over time. Specifically, the 6WMT, TUG, gait speed, WOMAC-pain, WOMAC-function, VAS, and EQ-5D scores showed a significant improvement at 1-month post-TKA, whereas SCT, peak torque of the knee extensors and flexors, and WOMAC-stiffness scores showed gradual, but substantial, improvements over 3 months. There were between-group differences (unilateral and bilateral TKA groups) in the time course of the SCT, 6MWT, TUG, VAS, WOAMC-stiffness, and WOMAC-function results.
CONCLUSION
Patients who underwent critical pathway rehabilitation after TKA showed significant improvements in functional measurements during the first 3 months post-surgery.
Keyword
MeSH Terms
Figure
-

Fig. 1. Flow chart of patient inclusion with reason for exclusion and total study population. CP, critical pathway; TKA, total knee arthroplasty.
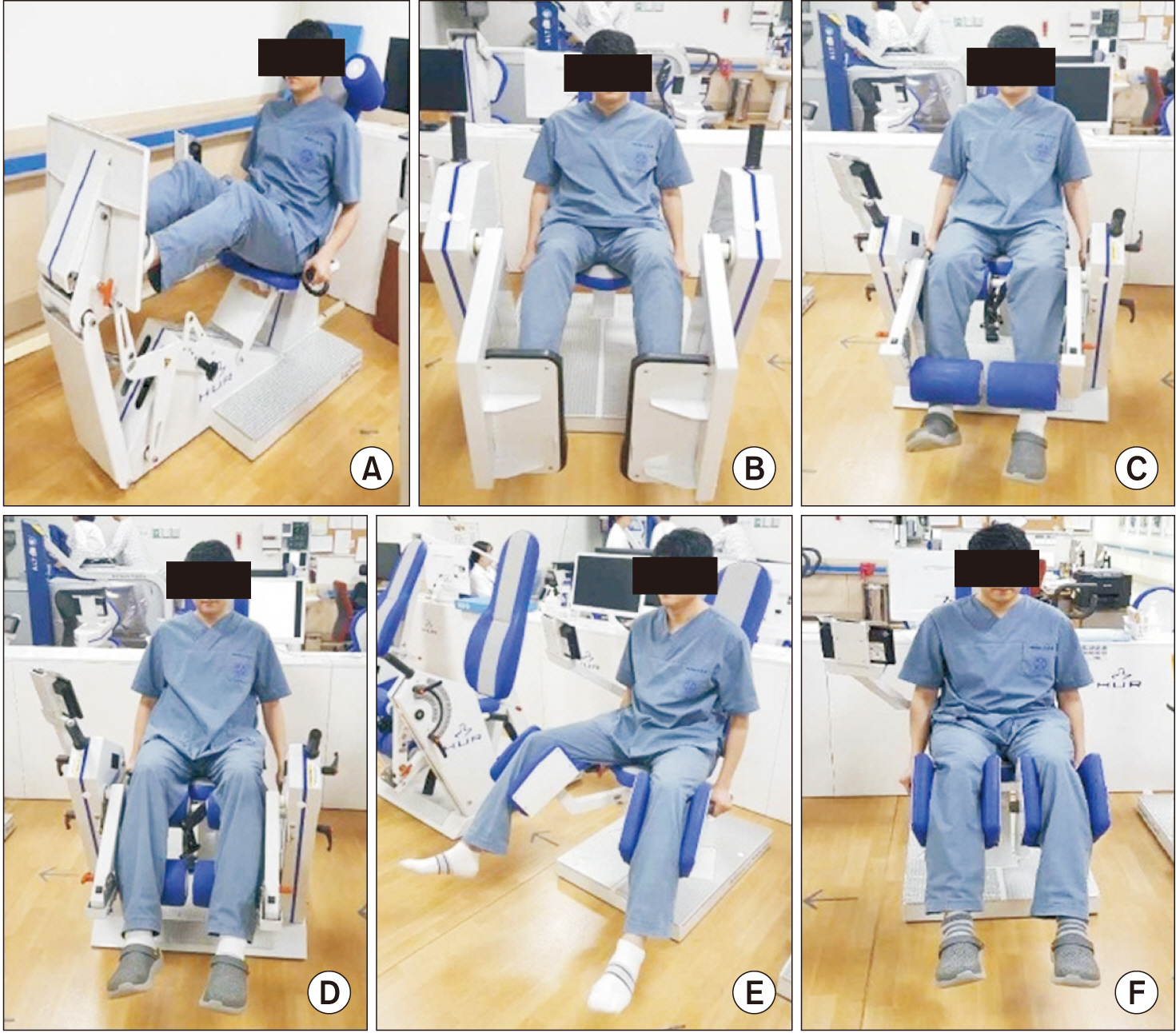
Fig. 2. The progressive resistance exercises consisted of (A) incline leg press, (B) leg press, (C) leg extension, (D) leg curl, (E) hip abduction, and (F) hip adduction using air-resistance machines (HUR Co., Kokkola, Finland).

Fig. 3. The gait training exercises consisted of Alter G anti-gravity treadmill (Model M320; Alter G Inc., Fremont, CA, USA).
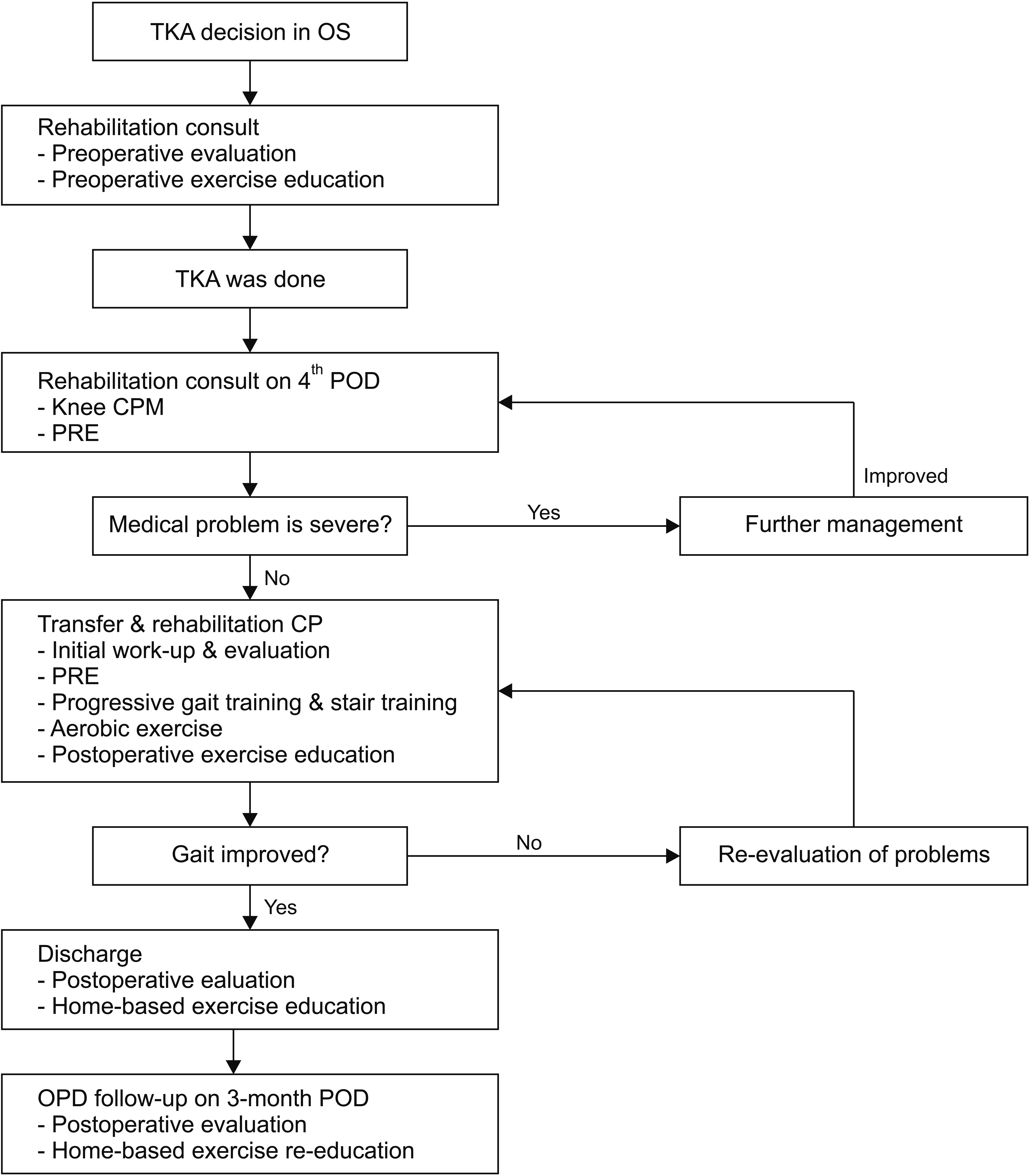
Fig. 4. Critical pathway after total knee arthroplasty. OS, orthopedic surgeon; TKA, total knee arthroplasty; POD, post-operation day; CPM, continuous passive motion; CP, critical pathway; PRE, progressive resistance exercise; OPD, outpatient department.
Reference
-
1. Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis. 2001; 60:91–7.
Article2. Cushnaghan J, Bennett J, Reading I, Croft P, Byng P, Cox K, et al. Long-term outcome following total knee arthroplasty: a controlled longitudinal study. Ann Rheum Dis. 2009; 68:642–7.
Article3. Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004; 86:963–74.4. Xie F, Lo NN, Pullenayegum EM, Tarride JE, O’Reilly DJ, Goeree R, et al. Evaluation of health outcomes in osteoarthritis patients after total knee replacement: a two-year follow-up. Health Qual Life Outcomes. 2010; 8:87.
Article5. Kehlet H, Thienpont E. Fast-track knee arthroplasty: status and future challenges. Knee. 2013; 20 Suppl 1:S29–33.6. Jakobsen TL, Kehlet H, Husted H, Petersen J, Bandholm T. Early progressive strength training to enhance recovery after fast-track total knee arthroplasty: a randomized controlled trial. Arthritis Care Res (Hoboken). 2014; 66:1856–66.
Article7. Bade MJ, Stevens-Lapsley JE. Early high-intensity rehabilitation following total knee arthroplasty improves outcomes. J Orthop Sports Phys Ther. 2011; 41:932–41.
Article8. Bade MJ, Kohrt WM, Stevens-Lapsley JE. Outcomes before and after total knee arthroplasty compared to healthy adults. J Orthop Sports Phys Ther. 2010; 40:559–67.
Article9. Walsh M, Woodhouse LJ, Thomas SG, Finch E. Physical impairments and functional limitations: a comparison of individuals 1 year after total knee arthroplasty with control subjects. Phys Ther. 1998; 78:248–58.
Article10. Buhagiar MA, Naylor JM, Harris IA, Xuan W, Kohler F, Wright R, et al. Effect of inpatient rehabilitation vs a monitored home-based program on mobility in patients with total knee arthroplasty: the HIHO randomized clinical trial. JAMA. 2017; 317:1037–46.11. Kang JH, Lee G, Kim KE, Lee YK, Lim JY. Determinants of functional outcomes using clinical pathways for rehabilitation after hip fracture surgery. Ann Geriatr Med Res. 2018; 22:26–32.
Article12. Duncan CM, Moeschler SM, Horlocker TT, Hanssen AD, Hebl JR. A self-paired comparison of perioperative outcomes before and after implementation of a clinical pathway in patients undergoing total knee arthroplasty. Reg Anesth Pain Med. 2013; 38:533–8.
Article13. Ribinik P, Le Moine F, de Korvin G, Coudeyre E, Genty M, Rannou F, et al. Physical and rehabilitation medicine (PRM) care pathways: “patients after total knee arthroplasty”. Ann Phys Rehabil Med. 2012; 55:533–9.
Article14. van der Sluis G, Goldbohm RA, Elings JE, Nijhuis-van der Sanden MW, Akkermans RP, Bimmel R, et al. Preoperative functional mobility as an independent determinant of inpatient functional recovery after total knee arthroplasty during three periods that coincided with changes in clinical pathways. Bone Joint J. 2017; 99-B:211–7.15. Ayalon O, Liu S, Flics S, Cahill J, Juliano K, Cornell CN. A multimodal clinical pathway can reduce length of stay after total knee arthroplasty. HSS J. 2011; 7:9–15.
Article16. Lenssen AF, Crijns YH, Waltje EM, van Steyn MJ, Geesink RJ, van den Brandt PA, et al. Efficiency of immediate postoperative inpatient physical therapy following total knee arthroplasty: an RCT. BMC Musculoskelet Disord. 2006; 7:71.
Article17. Almeida GJ, Schroeder CA, Gil AB, Fitzgerald GK, Piva SR. Interrater reliability and validity of the stair ascend/descend test in subjects with total knee arthroplasty. Arch Phys Med Rehabil. 2010; 91:932–8.
Article18. Enright PL, McBurnie MA, Bittner V, Tracy RP, McNamara R, Arnold A, et al. The 6-min walk test: a quick measure of functional status in elderly adults. Chest. 2003; 123:387–98.
Article19. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991; 39:142–8.20. Bugane F, Benedetti MG, Casadio G, Attala S, Biagi F, Manca M, et al. Estimation of spatial-temporal gait parameters in level walking based on a single accelerometer: validation on normal subjects by standard gait analysis. Comput Methods Programs Biomed. 2012; 108:129–37.21. Maffiuletti NA, Bizzini M, Desbrosses K, Babault N, Munzinger U. Reliability of knee extension and flexion measurements using the Con-Trex isokinetic dynamometer. Clin Physiol Funct Imaging. 2007; 27:346–53.
Article22. Thorstensson A, Karlsson J. Fatiguability and fibre composition of human skeletal muscle. Acta Physiol Scand. 1976; 98:318–22.
Article23. Cibere J, Bellamy N, Thorne A, Esdaile JM, McGorm KJ, Chalmers A, et al. Reliability of the knee examination in osteoarthritis: effect of standardization. Arthritis Rheum. 2004; 50:458–68.
Article24. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988; 15:1833–40.25. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983; 16:87–101.
Article26. Kim MH, Cho YS, Uhm WS, Kim S, Bae SC. Crosscultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual Life Res. 2005; 14:1401–6.
Article27. Benedetti MG, Sarti D, Stagni SB, Mariani E. Setting, clinical pathways, fast-track and rehabilitation following primary knee arthroplasty: a literature review. Open Rehabil J. 2015; 8:17–24.
Article28. Pennington JM, Jones DP, McIntyre S. Clinical pathways in total knee arthroplasty: a New Zealand experience. J Orthop Surg (Hong Kong). 2003; 11:166–73.
Article29. Judd DL, Eckhoff DG, Stevens-Lapsley JE. Muscle strength loss in the lower limb after total knee arthroplasty. Am J Phys Med Rehabil. 2012; 91:220–6.
Article30. Salmon P, Hall GM, Peerbhoy D, Shenkin A, Parker C. Recovery from hip and knee arthroplasty: Patients’ perspective on pain, function, quality of life, and wellbeing up to 6 months postoperatively. Arch Phys Med Rehabil. 2001; 82:360–6.
Article31. Moffet H, Collet JP, Shapiro SH, Paradis G, Marquis F, Roy L. Effectiveness of intensive rehabilitation on functional ability and quality of life after first total knee arthroplasty: a single-blind randomized controlled trial. Arch Phys Med Rehabil. 2004; 85:546–56.
Article32. Aalund PK, Larsen K, Hansen TB, Bandholm T. Normalized knee-extension strength or leg-press power after fast-track total knee arthroplasty: which measure is most closely associated with performance-based and self-reported function? Arch Phys Med Rehabil. 2013; 94:384–90.
Article33. Skoffer B, Dalgas U, Mechlenburg I, Soballe K, Maribo T. Functional performance is associated with both knee extensor and flexor muscle strength in patients scheduled for total knee arthroplasty: a cross-sectional study. J Rehabil Med. 2015; 47:454–9.
Article34. Brown K, Kachelman J, Topp R, Quesada PM, Nyland J, Malkani A, et al. Predictors of functional task performance among patients scheduled for total knee arthroplasty. J Strength Cond Res. 2009; 23:436–43.
Article35. Rossi MD, Brown LE, Whitehurst M. Knee extensor and flexor torque characteristics before and after unilateral total knee arthroplasty. Am J Phys Med Rehabil. 2006; 85:737–46.
Article36. Mizner RL, Petterson SC, Stevens JE, Vandenborne K, Snyder-Mackler L. Early quadriceps strength loss after total knee arthroplasty. The contributions of muscle atrophy and failure of voluntary muscle activation. J Bone Joint Surg Am. 2005; 87:1047–53.37. Iwata A, Sano Y, Wanaka H, Yamamoto S, Yano Y, Iwata H. Different improvement trends in gait function and quadriceps strength early after total knee arthroplasty. J Phys Ther Sci. 2019; 31:57–62.
Article38. Valtonen AM, Poyhonen T, Manninen M, Heinonen A, Sipila S. Knee extensor and flexor muscle power explains stair ascension time in patients with unilateral late-stage knee osteoarthritis: a cross-sectional study. Arch Phys Med Rehabil. 2015; 96:253–9.
Article39. Huang YH, Lin C, Yang JH, Lin LC, Mou CY, Chiang KT, et al. No difference in the functional improvements between unilateral and bilateral total knee replacements. BMC Musculoskelet Disord. 2018; 19:87.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acceptable Functional Outcomes and Patient Satisfaction Following Total Knee Arthroplasty in Asians with Severe Knee Stiffness: A Matched Analysis
- Evaluation of Postoperative Range of Motion and Functional Outcomes after Cruciate-Retaining and Posterior-Stabilized High-Flexion Total Knee Arthroplasty
- Efficacy of Physiotherapist after Total Knee Arthroplasty
- Evaluation of Muscle Strength Using Isokinetic Testing and Functional Result after Total Knee Arthroplasty
- Diabetes mellitus does not increase the risk of knee stiffness after total knee arthroplasty: a meta-analysis of 7 studies including 246 053 cases
