Feasibility and Applicability of Wireless Handheld Ultrasound Measurement of Carotid Intima-Media Thickness in Patients with Cardiac Symptoms
- Affiliations
-
- 1Department of Cardiovascular Medicine, Gachon University Gil Medical Center, Incheon, Korea. heart@gilhospital.com
- 2Gachon Cardiovascular Research Institute, Gachon University, Incheon, Korea.
- 3Department of Medical Engineering, School of Medicine, Gachon University, Incheon, Korea.
- 4Healcerion Co., Ltd., Seoul, Korea.
- KMID: 2468487
- DOI: http://doi.org/10.3349/ymj.2020.61.2.129
Abstract
- PURPOSE
Routine screening for carotid intima-media thickness (CIMT) and cardiovascular (CV) disease in asymptomatic patients has been criticized for the high costs and large number of patients required for detecting one patient with coronary artery disease (CAD). In order to overcome the low cost-effectiveness thereof, we investigated the feasibility of an economic wireless handheld ultrasound (WHUS) device for CIMT measurement in symptomatic patients.
MATERIALS AND METHODS
A total of 100 consecutive patients with cardiac symptoms were enrolled. CIMT was measured in all patients. Coronary angiography was performed in 75 patients indicated for the exam.
RESULTS
The mean of maximal CIMT measured from left/right common carotid artery and bulb (max-CIMT) by the WHUS device showed excellent agreement [intraclass correlation coefficient (ICC)=0.960] with a standard ultrasound device and great interobserver repeatability (ICC>0.9 between all observers). Receiver operating characteristic curve analysis showed that the predictive power for CAD was improved when max-CIMT and plaque information (plaque≥2) was added [area under the curve (AUC): 0.838] to the traditional clinical CV risk factors (AUC: 0.769). The cutoff values for CAD prediction with the standard device and the WHUS device were 1.05 mm (AUC: 0.807, sensitivity: 0.78, specificity: 0.53) and 1.10 mm (AUC: 0.725, sensitivity: 0.98, specificity: 0.27), respectively.
CONCLUSION
max-CIMT measured by a WHUS device showed excellent agreement and repeatability, compared with standard ultrasound. Combined max-CIMT and plaque information added predictive power to the traditional clinical CV risk factors in detecting high-risk CAD patients.
Keyword
MeSH Terms
Figure
-
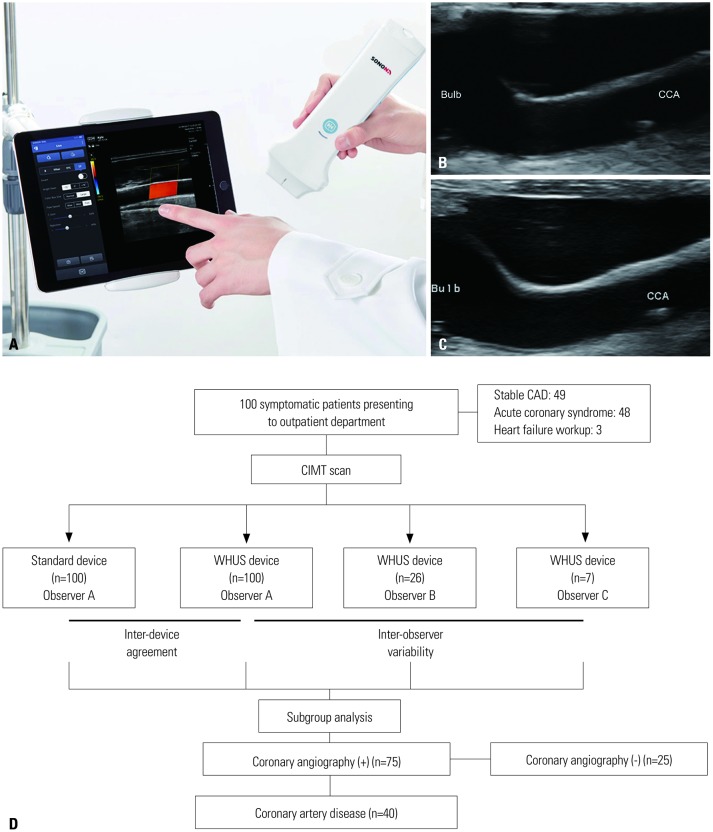
Fig. 1 Images of the WHUS device, carotid scans from both devices, and details on patient enrollment. (A) The WHUS device can be connected to cellphones or tablets through its built-in Wi-Fi feature from virtually anywhere. The carotid bulb and CCA of the same patient acquired by the (B) WHUS and (C) standard device. (D) The carotid intima-media thickness of a total of 100 patients with cardiac symptoms was evaluated both by the standard and WHUS devices. WHUS, wireless handheld ultrasound; CIMT, carotid intima-media thickness; CAD, coronary artery disease; CCA, common carotid artery.
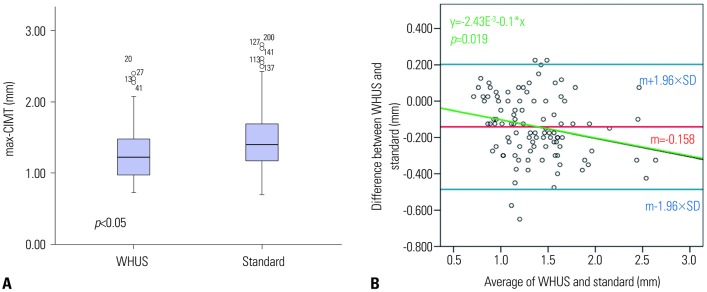
Fig. 2 Interdevice agreement and proportional bias. (A) A plot showing the CIMT of the WHUS and the standard device. (B) A Bland-Altman plot of the relationship between the average of WHUS and standard device and differences between the two devices. m, mean of differences between the WHUS and standard device; max-CIMT, mean of the maximal values of carotid intima-medial thickness of a patient; WHUS, wireless handheld ultrasound.
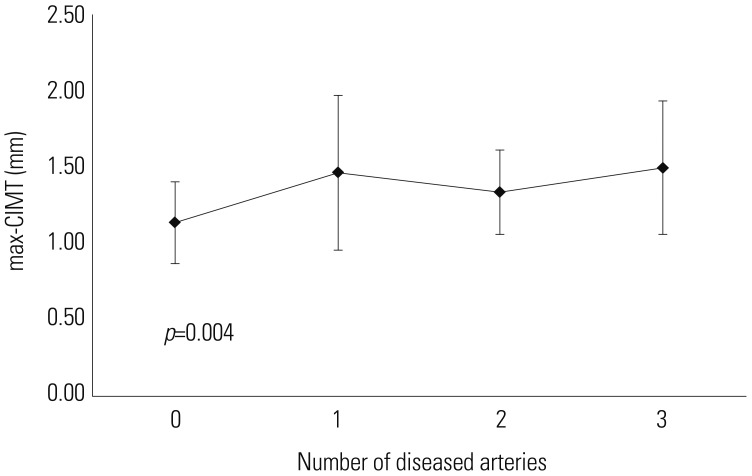
Fig. 3 Relationship between maximal carotid intima-media thickness (max-CIMT) and the number of each patient's diseased coronary vessels.
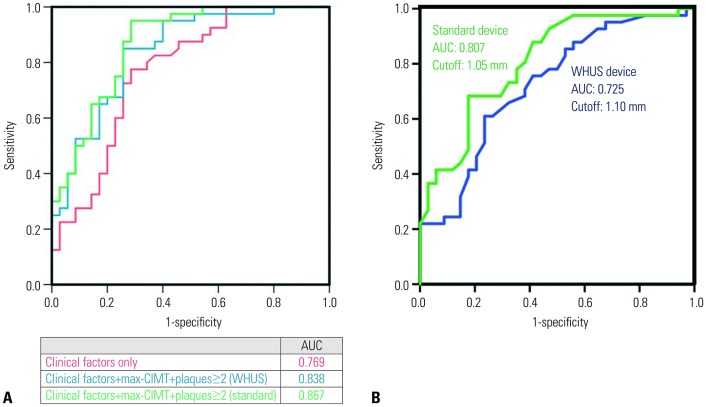
Fig. 4 ROC curves for predicting high-risk CAD patients. (A) A plot showing the predictive power of traditional clinical risk factors alone (red), mean maximal CIMT measured from left/right CCA and bulb (max-CIMT), and carotid plaques ≥2, in addition to clinical risk factors, using the WHUS and the standard device, shown in blue and green, respectively. (B) The cutoff max-CIMT values and in predicting high-risk CAD patients using the standard (1.05 mm) and WHUS (1.10 mm) device. ROC, receiver operating characteristic; AUC, area under the curve; CAD, coronary artery disease; WHUS, wireless hand-held ultrasound.
Reference
-
1. Nambi V, Chambless L, Folsom AR, He M, Hu Y, Mosley T, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol. 2010; 55:1600–1607. PMID: 20378078.2. Cao JJ, Arnold AM, Manolio TA, Polak JF, Psaty BM, Hirsch CH, et al. Association of carotid artery intima-media thickness, plaques, and C-reactive protein with future cardiovascular disease and all-cause mortality: the Cardiovascular Health Study. Circulation. 2007; 116:32–38. PMID: 17576871.3. Øygarden H. Carotid intima-media thickness and prediction of cardiovascular disease. J Am Heart Assoc. 2017; 6:e005313. PMID: 28110312.
Article4. Zanchetti A, Hennig M, Hollweck R, Bond G, Tang R, Cuspidi C, et al. Baseline values but not treatment-induced changes in carotid intima-media thickness predict incident cardiovascular events in treated hypertensive patients: findings in the European Lacidipine Study on Atherosclerosis (ELSA). Circulation. 2009; 120:1084–1090. PMID: 19738145.5. Kwon HJ, Park JH, Lee JH, Jeong HS, Song HJ, Kim J, et al. Low common carotid artery systolic occlusion pressure and symptomatic carotid artery stenosis are associated with development of neurologic intolerance during proximal protected carotid artery stenting. Korean Circ J. 2018; 48:217–226. PMID: 29557108.
Article6. Dwivedi A, Al'Aref SJ, Lin FY, Min JK. Evaluation of atherosclerotic plaque in non-invasive coronary imaging. Korean Circ J. 2018; 48:124–133. PMID: 29441745.
Article7. Bots ML, Groenewegen KA, Anderson TJ, Britton AR, Dekker JM, Engström G, et al. Common carotid intima-media thickness measurements do not improve cardiovascular risk prediction in individuals with elevated blood pressure: the USE-IMT collaboration. Hypertension. 2014; 63:1173–1181. PMID: 24614213.8. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39:3021–3104. PMID: 30165516.
Article9. Costanzo P, Perrone-Filardi P, Vassallo E, Paolillo S, Cesarano P, Brevetti G, et al. Does carotid intima-media thickness regression predict reduction of cardiovascular events? A meta-analysis of 41 randomized trials. J Am Coll Cardiol. 2010; 56:2006–2020. PMID: 21126642.
Article10. Lorenz MW, Polak JF, Kavousi M, Mathiesen EB, Völzke H, Tuomainen TP, et al. Carotid intima-media thickness progression to predict cardiovascular events in the general population (the PROG-IMT collaborative project): a meta-analysis of individual participant data. Lancet. 2012; 379:2053–2062. PMID: 22541275.
Article11. den Ruijter HM, Vaartjes I, Sutton-Tyrrell K, Bots ML, Koffijberg H. Long-term health benefits and costs of measurement of carotid intima-media thickness in prevention of coronary heart disease. J Hypertens. 2013; 31:782–790. PMID: 23442989.
Article12. Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB Sr, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:2935–2959. PMID: 24239921.13. Kim EY, Park KH, Choi SJ, Chung WJ. Educational value of pocket-sized ultrasound devices to improve understanding of ultrasound examination principles and sonographic anatomy for medical student. PLoS One. 2017; 12:e0185031. PMID: 28961257.
Article14. Lee SH, Kim YJ. Managing a seroma with wireless mobile ultrasound device. J Plast Reconstr Aesthet Surg. 2017; 70:e7–e9. PMID: 28010935.
Article15. Kim J, Kim S, Jeon S, Jung S. A longitudinal study investigating cervical changes during labor using a wireless ultrasound device. J Matern Fetal Neonatal Med. 2018; 31:1787–1791. PMID: 28627262.
Article16. Oh NR, Woo JH, Kim DY, Baek MK. Wireless mobile ultrasonography-assisted parotid duct stone removal. Ear Nose Throat J. 2018; 97:E36–E38.
Article17. Dogan S, Kastelein JJ, Grobbee DE, Bots ML. Mean common or mean maximum carotid intima-media thickness as primary outcome in lipid-modifying intervention studies. J Atheroscler Thromb. 2011; 18:946–957. PMID: 21844660.
Article18. Seo J, Kim GS, Lee HY, Byun YS, Jung IH, Rhee KJ, et al. Prevalence and clinical outcomes of asymptomatic carotid artery stenosis in patients undergoing concurrent coronary and carotid angiography. Yonsei Med J. 2019; 60:542–546. PMID: 31124337.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carotid ultrasound in patients with coronary artery disease
- Do we need individual measurement of carotid intima and media thickness?
- Measurements of Carotid Intima, Media, and Intima-media Thickness and Their Clinical Importance
- Response: Increased Carotid Intima-Media Thickness Is Associated with Progression of Diabetic Nephropathy in Patients with Type 2 Diabetes
- Measurement of the Carotid Intima, Media and Intima-Media Thickness with Ultrasound and New Software
