Left Ventricular Filling Pressure as Assessed by the E/e' Ratio Is a Determinant of Atrial Fibrillation Recurrence after Cardioversion
- Affiliations
-
- 1Cardiology Division, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. JYKIM0706@yuhs.ac
- KMID: 2466353
- DOI: http://doi.org/10.3349/ymj.2016.57.1.64
Abstract
- PURPOSE
Left ventricular (LV) filling pressure affects atrial fibrillation (AF) recurrence. We investigated the relationship between diastolic dysfunction and AF recurrence after cardioversion, and whether LV filling pressure was predictive of AF recurrence.
MATERIALS AND METHODS
Sixty-six patients (mean 58+/-12 years) with newly diagnosed persistent AF were retrospectively enrolled. We excluded patients with left atrial (LA) diameters larger than 50 mm, thereby isolating the effect of LV filling pressure. We evaluated the differences between the patients with (group 1) and without AF recurrence (group 2).
RESULTS
Group 1 showed increased LA volume index (LAVI) and E/e' compared to group 2 (p<0.05). During a mean follow-up period of 25+/-19 months, AF recurrence after cardioversion was 60.6% (40/66). The area under the receiver operating characteristics curve of E/e' for AF recurrence was 0.780 [95% confidence interval (CI): 0.657-0.903], and the optimal cut-off value of the E/e' was 9.15 with 75.0% of sensitivity and 73.1% of specificity. A Kaplan-Meier survival curve showed that the cumulative recurrence-free survival rate was significantly lower in patients with higher LV filling pressure (E/e'>9.15) compared with patients with lower LV filling pressure (E/e'< or =9.15) (log rank p=0.008). Cox regression analysis revealed that E/e' [hazards ratio (HR): 1.100, 95% CI: 1.017-1.190] and LAVI (HR: 1.042, 95% CI: 1.002-1.084) were independent predictors for AF recurrence after cardioversion.
CONCLUSION
LV filling pressure predicts the risk of AF recurrence in persistent AF patients after cardioversion.
Keyword
MeSH Terms
-
Aged
Atrial Fibrillation/*physiopathology
Electric Countershock
Female
Follow-Up Studies
Heart Atria/pathology/physiopathology
Humans
Kaplan-Meier Estimate
Male
Middle Aged
Proportional Hazards Models
ROC Curve
Recurrence
Regression Analysis
Retrospective Studies
Sensitivity and Specificity
Survival Rate
Ventricular Dysfunction, Left/*physiopathology
Figure
-

Fig. 1 The representative cases which reveal the difference of E/e' between two groups. (A) In patients without recurrence, early (E) diastolic mitral inflow peak velocity and early diastolic mitral annulus peak velocity (e') were measured, and the ratio of E/e' was calculated. (B) In patients with recurrence, the ratio of E/e' was calculated by the same way.
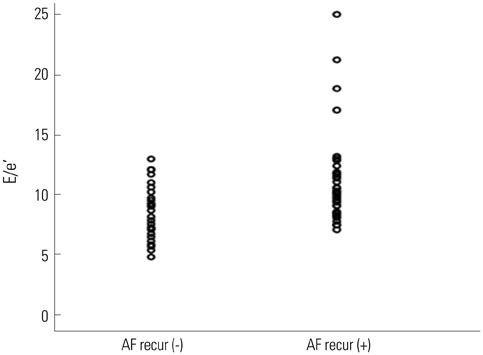
Fig. 2 The scatter plots of E/e' with or without AF recurrence. AF, atrial fibrillation; E/e', the ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e').
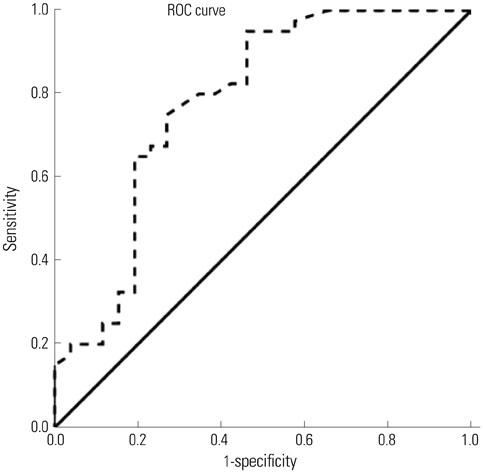
Fig. 3 Receiver operating characteristic (ROC) curves for E/e' for AF recurrence after cardioversion. Area under the ROC curve for E/e' was 0.780 (95% confidence interval: 0.657-0.903, p<0.001). AF, atrial fibrillation; E/e', the ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e').

Fig. 4 The Kaplan-Meier survival curves for AF recurrence in patients after cardioversion with or without increased LV filling pressure. AF, atrial fibrillation; E/e', the ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e'); LV, left ventricle.
Reference
-
1. European Heart Rhythm Association. European Association for Cardio-Thoracic Surgery. Camm AJ, Kirchhof P, Lip GY, Schotten U, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010; 31:2369–2429.2. Melduni RM, Cullen MW. Role of left ventricular diastolic dysfunction in predicting atrial fibrillation recurrence after successful electrical cardioversion. J Atr Fibrillation. 2012; 5:87–94.3. Huang JL, Tai CT, Lin YJ, Ting CT, Chen YT, Chang MS, et al. The mechanisms of an increased dominant frequency in the left atrial posterior wall during atrial fibrillation in acute atrial dilatation. J Cardiovasc Electrophysiol. 2006; 17:178–188.
Article4. Caputo M, Urselli R, Capati E, Navarri R, Sinesi L, Furiozzi F, et al. Usefulness of left ventricular diastolic dysfunction assessed by pulsed tissue Doppler imaging as a predictor of atrial fibrillation recurrence after successful electrical cardioversion. Am J Cardiol. 2011; 108:698–704.
Article5. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011; 123:e269–e367.6. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.
Article7. Prystowsky EN, Benson DW Jr, Fuster V, Hart RG, Kay GN, Myerburg RJ, et al. Management of patients with atrial fibrillation. A statement for healthcare professionals. From the subcommittee on electrocardiography and electrophysiology, American Heart Association. Circulation. 1996; 93:1262–1277.8. Kim H, Lee JP, Yoon HJ, Park HS, Cho YK, Nam CW, et al. Association between Doppler flow of atrial fibrillatory contraction and recurrence of atrial fibrillation after electrical cardioversion. J Am Soc Echocardiogr. 2014; 27:1107–1112.
Article9. Okura H, Takada Y, Kubo T, Iwata K, Mizoguchi S, Taguchi H, et al. Tissue Doppler-derived index of left ventricular filling pressure, E/E', predicts survival of patients with non-valvular atrial fibrillation. Heart. 2006; 92:1248–1252.
Article10. Bolognesi R, Tsialtas D, Barilli AL, Manca C, Zeppellini R, Javernaro A, et al. Detection of early abnormalities of left ventricular function by hemodynamic, echo-tissue Doppler imaging, and mitral Doppler flow techniques in patients with coronary artery disease and normal ejection fraction. J Am Soc Echocardiogr. 2001; 14:764–772.
Article11. Watanabe T, Iwai-Takano M, Oikawa M, Yamaki T, Yaoita H, Maruyama Y. Optimal noninvasive assessment of diastolic heart failure in patients with atrial fibrillation: comparison of tissue doppler echocardiography, left atrium size, and brain natriuretic peptide. J Am Soc Echocardiogr. 2008; 21:689–696.
Article12. Khan A, Moe GW, Nili N, Rezaei E, Eskandarian M, Butany J, et al. The cardiac atria are chambers of active remodeling and dynamic collagen turnover during evolving heart failure. J Am Coll Cardiol. 2004; 43:68–76.
Article13. Chin JY, Youn HJ. The effect of ablation for paroxysmal atrial fibrillation on left atrial volume and function: a one-year follow-up study. Yonsei Med J. 2014; 55:895–903.
Article14. Tsang TS, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Left atrial volume as a morphophysiologic expression of left ventricular diastolic dysfunction and relation to cardiovascular risk burden. Am J Cardiol. 2002; 90:1284–1289.
Article15. Kojima T, Kawasaki M, Tanaka R, Ono K, Hirose T, Iwama M, et al. Left atrial global and regional function in patients with paroxysmal atrial fibrillation has already been impaired before enlargement of left atrium: velocity vector imaging echocardiography study. Eur Heart J Cardiovasc Imaging. 2012; 13:227–234.
Article16. Lancellotti P, Henri C. The left atrium: an old 'barometer' which can reveal great secrets. Eur J Heart Fail. 2014; 16:1047–1048.
Article17. Olshansky B, Heller EN, Mitchell LB, Chandler M, Slater W, Green M, et al. Are transthoracic echocardiographic parameters associated with atrial fibrillation recurrence or stroke? Results from the atrial fibrillation follow-up investigation of rhythm management (AFFIRM) study. J Am Coll Cardiol. 2005; 45:2026–2033.
Article18. Schneider MP, Hua TA, Böhm M, Wachtell K, Kjeldsen SE, Schmieder RE. Prevention of atrial fibrillation by Renin-Angiotensin system inhibition a meta-analysis. J Am Coll Cardiol. 2010; 55:2299–2307.
Article19. Fukuda Y, Fukuda N, Morishita S, Tamura Y. Preventive effect of renin-angiotensin system inhibitor on left atrial remodelling in patients with chronic atrial fibrillation: long-term echocardiographic study. Eur J Echocardiogr. 2011; 12:278–282.20. ACTIVE I Investigators. Yusuf S, Healey JS, Pogue J, Chrolavicius S, Flather M, et al. Irbesartan in patients with atrial fibrillation. N Engl J Med. 2011; 364:928–938.
Article21. GISSI-AF Investigators. Disertori M, Latini R, Barlera S, Franzosi MG, Staszewsky L, et al. Valsartan for prevention of recurrent atrial fibrillation. N Engl J Med. 2009; 360:1606–1617.
Article22. Ishikawa K, Yamada T, Yoshida Y, Takigawa M, Aoyama Y, Inoue N, et al. Renin-angiotensin system blocker use may be associated with suppression of atrial fibrillation recurrence after pulmonary vein isolation. Pacing Clin Electrophysiol. 2011; 34:296–303.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Influence of Electrical Cardioversion for Atrial Fibrillation on Left Atrial Appendage Function: A Transesophageal Echocardiography Study
- Atrial Fibrillation in a Patient with Left Ventricular Hypertrophy after Induction of General Anesthesia: A case report
- A clinical observation on antiarrhythmic efficacy of propafenone for atrial fibrillation
- The Influence of the Left Ventricular Geometry on the Left Atrial Size and Left Ventricular Filling Pressure in Hypertensive Patients, as Assessed by Echocardiography
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
