Brown-Séquard Syndrome Caused by Acute Traumatic Cervical Disc Herniation
- Affiliations
-
- 1Department of Neurosurgery, Chungdam Wooridul Spine Hospital, Seoul, Korea. anconeus@daum.net
- KMID: 2461129
- DOI: http://doi.org/10.13004/kjnt.2019.15.e21
Abstract
- Brown-Séquard syndrome (BSS) is an incomplete spinal cord injury caused by damage to one-half of the spinal cord. Most cases of BSS result from penetrating trauma or tumors, and acute cervical disc herniation is a relatively rare cause of BSS. In this case, a 34-year-old man with a sudden onset posterior neck pain and left side motor weakness was admitted to the local spine hospital. Pain and temperature sensation of pain was decreased below the right C4 dermatome. The left arm and leg motor grade was 0. Magnetic resonance imaging (MRI) showed a huge trans-ligamentous herniated disc rupture from the center to the left at the level of C3-4, and anterior cervical discectomy and fusion were performed. After emergency surgery, left arm and leg motor grade recovered to 2, and normal voiding function returned. MRI verified complete removal of the cervical herniated disc. This case describes the approach to rapid diagnosis in a patient with characteristic clinical symptoms of BSS and radiological findings of a herniated cervical disc. Rapid and accurate diagnosis and immediate decompressive surgery increased the possibility of a good surgical outcome, even if the neurologic deficits are grave at the time of admission.
MeSH Terms
Figure
-
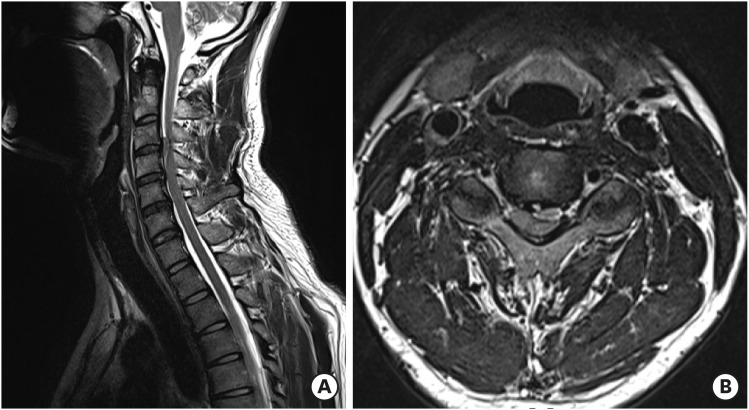
FIGURE 1 Preoperative cervical MRI. Sagittal (A) MRI shows a herniated disc at the C3–4 level. Axial (B) MRI shows a huge transligamentous disc rupture from the center to the left at the C3–4 level. Findings indicating contusion were also observed.MRI: magnetic resonance imaging.
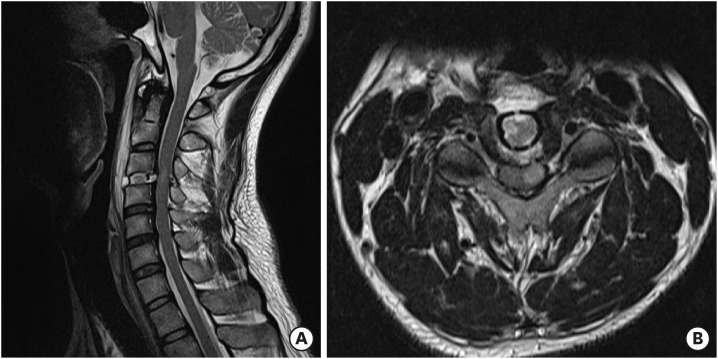
FIGURE 2 Postoperative cervical MRI. Sagittal (A) and axial (B) MRI shows a properly inserted cage and complete removal of the disc at C3–4. Signal changes persist in the left spinal cord.MRI: magnetic resonance imaging.
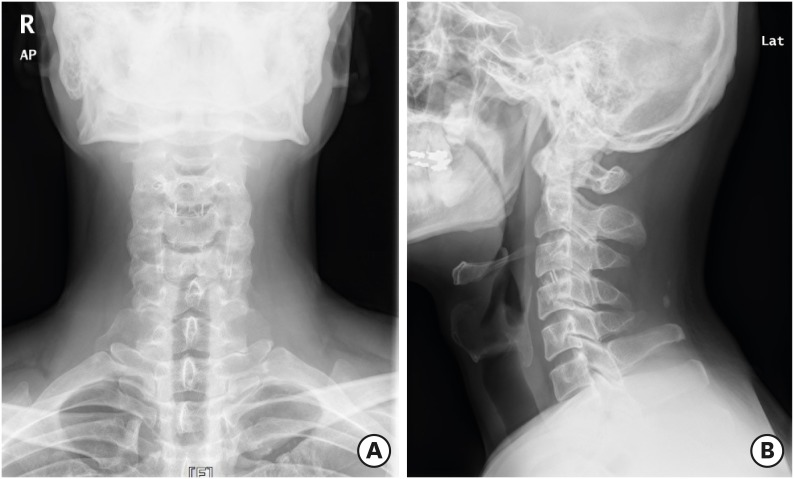
FIGURE 3 Cervical X-ray images 6 months after surgery. Cervical anteroposterior (A) and lateral (B) X-ray images show a well-maintained cage at the C3–4 level.
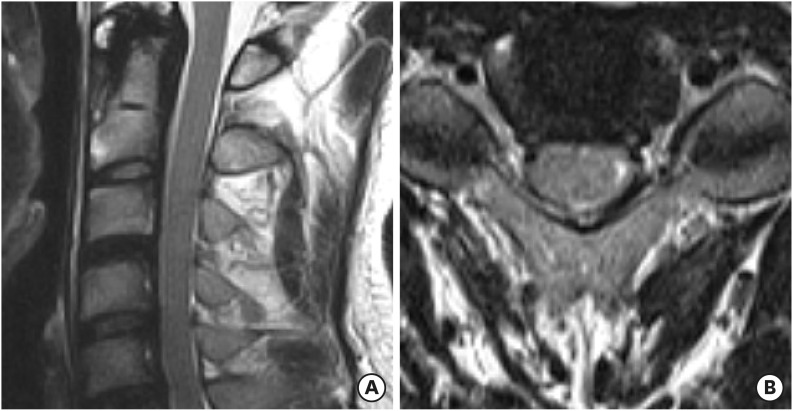
FIGURE 4 Cervical MRI 6 months after surgery. Sagittal (A) and axial (B) MRI shows fusion of C3–4 and decreased signal change in the spinal cord at C3–4.MRI: magnetic resonance imaging.
Reference
-
1. Aryan HE, Farin A, Nakaji P, Imbesi SG, Abshire BB. Intramedullary spinal cord metastasis of lung adenocarcinoma presenting as Brown-Sequard syndrome. Surg Neurol. 2004; 61:72–76. PMID: 14706385.
Article2. Choi KB, Lee CD, Chung DJ, Lee SH. Cervical disc herniation as a cause of brown-séquard syndrome. J Korean Neurosurg Soc. 2009; 46:505–510. PMID: 20041066.
Article3. Guan D, Wang G, Clare M, Kuang Z. Brown-Sequard syndrome produced by calcified herniated cervical disc and posterior vertebral osteophyte: Case report. J Orthop. 2015; 12:S260–S263. PMID: 27047233.
Article4. Kohno M, Takahashi H, Yamakawa K, Ide K, Segawa H. Postoperative prognosis of Brown-Séquard-type myelopathy in patients with cervical lesions. Surg Neurol. 1999; 51:241–246. PMID: 10086485.
Article5. McKinley W, Santos K, Meade M, Brooke K. Incidence and outcomes of spinal cord injury clinical syndromes. J Spinal Cord Med. 2007; 30:215–224. PMID: 17684887.
Article6. Meng Y, Zhou L, Liu X, Wang H, Shi J, Guo Y. Brown-sequard syndrome associated with horner syndrome following cervical disc herniation. Spinal Cord Ser Cases. 2016; 2:16037.
Article7. Moskowitz E, Schroeppel T. Brown-sequard syndrome. Trauma Surg Acute Care Open. 2018; 3:e000169. PMID: 29766141.
Article8. Pollard ME, Apple DF. Factors associated with improved neurologic outcomes in patients with incomplete tetraplegia. Spine (Phila Pa 1976). 2003; 28:33–39. PMID: 12544952.
Article9. Porto GB, Tan LA, Kasliwal MK, Traynelis VC. Progressive Brown-Séquard syndrome: a rare manifestation of cervical disc herniation. J Clin Neurosci. 2016; 29:196–198. PMID: 26921137.
Article10. Pouw MH, van de Meent H, van Middendorp JJ, Hirschfeld S, Thietje R, van Kampen A, et al. Relevance of the diagnosis traumatic cervical Brown-Séquard-plus syndrome: an analysis based on the neurological and functional recovery in a prospective cohort of 148 patients. Spinal Cord. 2010; 48:614–618. PMID: 20065980.
Article11. Roth EJ, Park T, Pang T, Yarkony GM, Lee MY. Traumatic cervical Brown-Sequard and Brown-Sequard-plus syndromes: the spectrum of presentations and outcomes. Paraplegia. 1991; 29:582–589. PMID: 1787982.
Article12. Sayer FT, Vitali AM, Low HL, Paquette S, Honey CR. Brown-Sèquard syndrome produced by C3-C4 cervical disc herniation: a case report and review of the literature. Spine (Phila Pa 1976). 2008; 33:E279–E282. PMID: 18427307.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extradural Cervical Disc Herniation Causing Sudden Brown-se'quard Syndrome: A Case Report
- Brown-Séquard Syndrome and Cervical Vertebral Fractures after Blunt Cervical Trauma in a Traffic Accident - A Case Report -
- Brown Sequard Syndrome Resulting from Cervical Disc Herniation Treated by Anterior Foraminotomy
- Cervical Spinal Cord Infarction Presenting Brown-Séquard-plus Syndrome
- Motion Preserving Surgery in Two Cases of Brown-Sequard Syndrome Caused by Herniated Cervical Discs
