Radiographic manifestations of fibroblastic osteosarcoma: A diagnostic challenge
- Affiliations
-
- 1Department of Diagnostic Sciences, Texas A&M University College of Dentistry, Dallas, TX, USA. tahmasbi@tamu.edu
- 2Department of Oral and Maxillofacial Surgery, Texas A&M University College of Dentistry, Dallas, TX, USA.
- KMID: 2458373
- DOI: http://doi.org/10.5624/isd.2019.49.3.235
Abstract
- Osteosarcoma is the most common primary bone tumor after plasma cell neoplasms. Osteosarcoma has diverse histological features and is characterized by the presence of malignant spindle cells and pluripotent neoplastic mesenchymal cells that produce immature bone, cartilage, and fibrous tissue. Osteosarcoma most frequently develops in the extremities of long bones, but can occur in the jaw in rare cases. The clinical and biological behavior of osteosarcoma of the jaw slightly differs from that of long-bone osteosarcoma. The incidence of jaw osteosarcoma is greater in the third to fourth decades of life, whereas long-bone osteosarcoma mostly occurs in the second decade of life. Osteosarcoma of the jaw has a lower tendency to metastasize and a better prognosis than long-bone osteosarcoma. Radiographically, osteosarcoma can present as a poorly-defined lytic, sclerotic, or mixed-density lesion with periosteal bone reaction response. Multi-detector computed tomography is useful for identifying the extent of bone destruction, as well as soft tissue involvement of the lesion. The current case report presents a fibroblastic osteosarcoma involving the left hemimandible with very unusual radiographic features.
Keyword
MeSH Terms
Figure
-

Fig. 1 Panoramic radiograph shows poorly defined osteolytic lesion involving the left hemimandible and ramus. Distruction of the inferior border of the mandible can be noted (arrow).
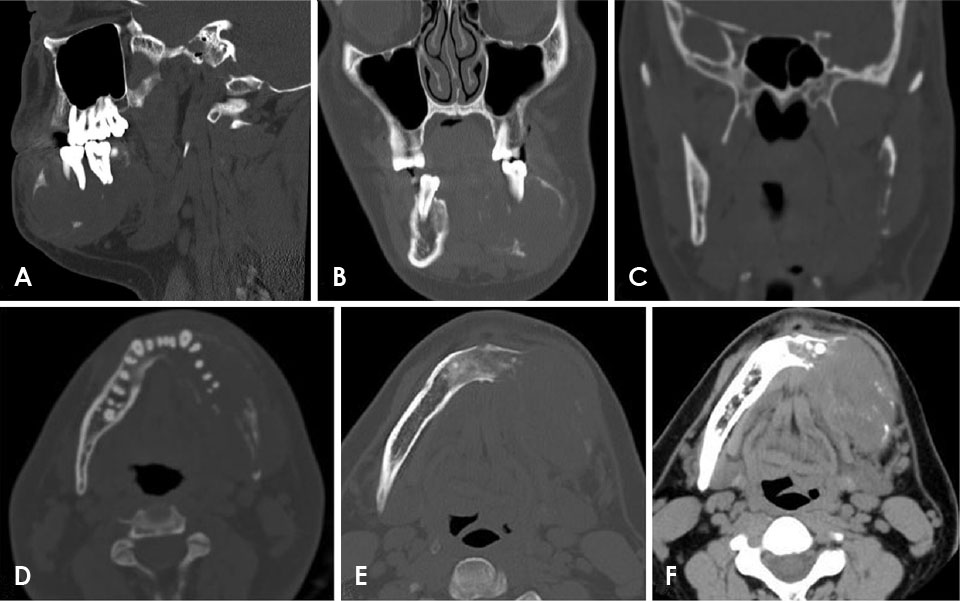
Fig. 2 Multi-detector computed tomographic imaging features of osteosarcoma of the left hemimandible. A. A sagittal bone-window image shows significant destruction of the body of the mandible, as well as scalloping of the margins. The mandibular first and second molars appear to be floating in air. B and C. Coronal bone-window images reveal an expansile destructive mass involving the mandible with significant destruction of the ramus. Axial bone-window images (D and E) and an axial soft tissue-window image (F) demonstrate significant destruction of the mandible, with an associated soft tissue mass. Facial asymmetry on the left side and asymmetric thickening of the overlying platysma muscle can be noted.
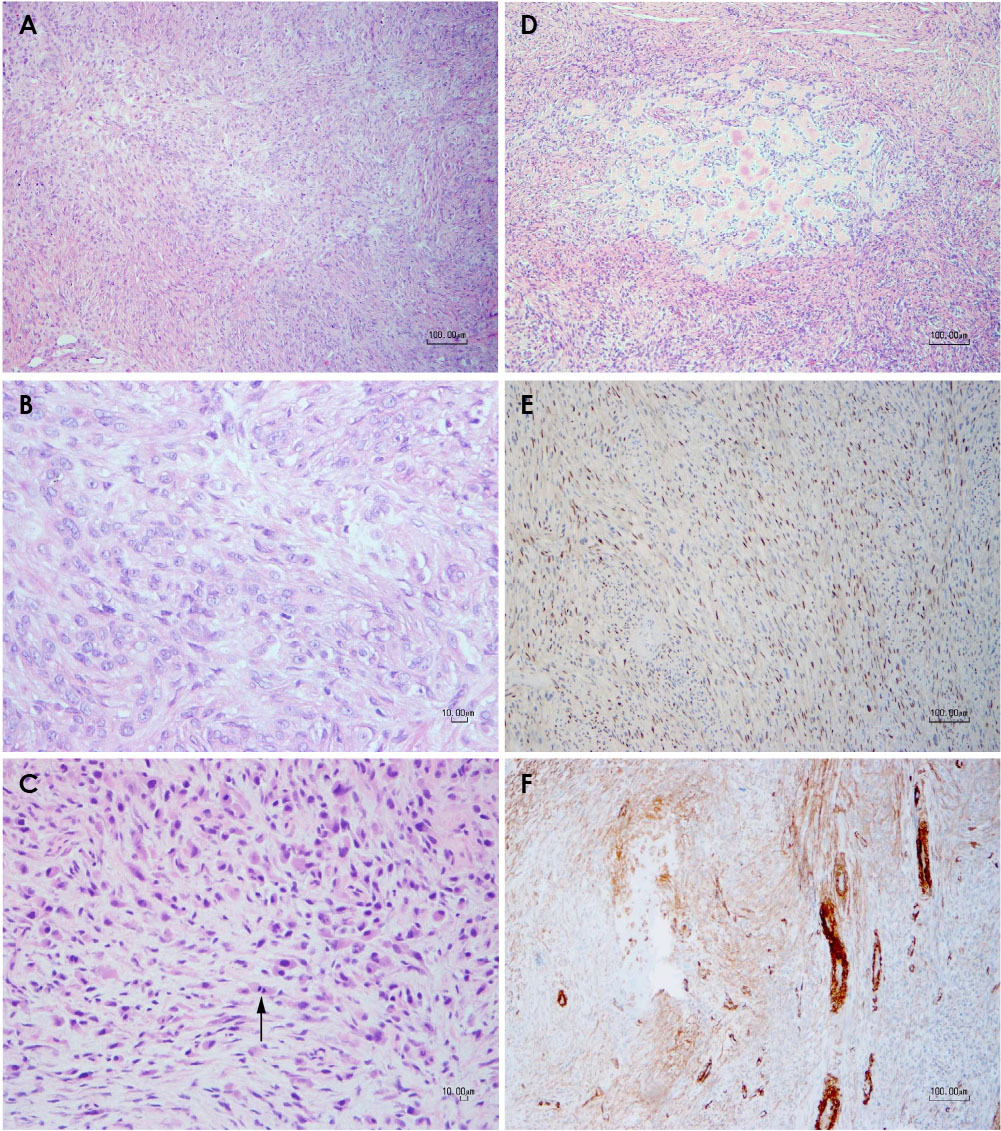
Fig. 3 Histologic and immunohistochemical findings of the incisional biopsy and the surgical resection specimen. A. Low-power view of the incisional biopsy shows a vaguely storiform pattern (hematoxylin and eosin [H&E], original magnification ×70). B. High-power view of the incisional biopsy, showing the bland cytomorphology of the spindle cells with indistinct cell borders (H&E, original magnification ×280). C. The surgical specimen demonstrates plump spindle cells showing hyperchromatic nuclei, pleomorphism, and a few mitotic figures (arrow), which are not seen in the incisional biopsy (H&E, original magnification ×140). D. Areas of the surgical specimen demonstrated osteoid formation (H&E, original magnification ×70). E. Immunohistochemical stain for SATB2 showed scattered nuclear positivity (original magnification ×70). F. Immunohistochemical stain for smooth muscle actin showed focal positivity, with more obvious staining in areas near the periphery of the tumor. The smooth muscle walls of the blood vessels served as an internal control (original magnification ×70).
Reference
-
1. Chaudhary M, Chaudhary SD. Osteosarcoma of jaws. J Oral Maxillofac Pathol. 2012; 16:233–238.
Article2. Amini Shakib P, Foroughi R, Seyedmajidi M. Osteosarcoma of the maxilla: a rare case with unusual clinical presentation. J Dent Res Dent Clin Dent Prospects. 2013; 7:177–181.3. Wadhwa N. Osteosarcoma: diagnostic dilemmas in histopathology and prognostic factors. Indian J Orthop. 2014; 48:247–254.
Article4. Ajura AJ, Lau SH. A retrospective clinicopathological study of 59 osteogenic sarcoma of jaw bone archived in a stomatology unit. Malays J Pathol. 2010; 32:27–34.5. Babazade F, Mortazavi H, Jalalian H. Bilateral metachronous osteosarcoma of the mandibular body: a case report. Chang Gung Med J. 2011; 34:6 Suppl. 66–69.6. Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. Cancer Treat Res. 2009; 152:3–13.
Article7. Wang S, Shi H, Yu Q. Osteosarcoma of the jaws: demographic and CT imaging features. Dentomaxillofac Radiol. 2012; 41:37–42.
Article8. Kalburge JV, Sahuji SK, Kalburge V, Kini Y. Osteosarcoma of mandible. J Clin Diagn Res. 2012; 6:1597–1599.
Article9. Sinha R, Roy Chowdhury SK, Chattopadhyay PK, Rajkumar K. Low-grade osteosarcoma of the mandible. J Maxillofac Oral Surg. 2010; 9:186–190.
Article10. Unni KK, Dahlin DC. Grading of bone tumors. Semin Diagn Pathol. 1984; 1:165–172.11. Bojan A, Christy W, Chanmougananda S, Ashokan K. Osteosarcoma of mandible: a case report and review of literature. J Clin Diagn Res. 2012; 6:753–757.12. Kundu ZS. Classification, imaging, biopsy and staging of osteosarcoma. Indian J Orthop. 2014; 48:238–246.
Article13. Horvai A, Unni KK. Premalignant conditions of bone. J Orthop Sci. 2006; 11:412–423.
Article14. Doganavsargil B, Argin M, Kececi B, Sezak M, Sanli UA, Oztop F. Secondary osteosarcoma arising in fibrous dysplasia, case report. Arch Orthop Trauma Surg. 2009; 129:439–444.
Article15. Takahashi S, Okada K, Nagasawa H, Shimada Y, Sakamoto H, Itoi E. Osteosarcoma occurring in osteogenesis imperfecta. Virchows Arch. 2004; 444:454–458.
Article16. Kassir RR, Rassekh CH, Kinsella JB, Segas J, Carrau RL, Hokanson JA. Osteosarcoma of the head and neck: meta-analysis of nonrandomized studies. Laryngoscope. 1997; 107:56–61.
Article17. Uysal KM, Koyuncuoğlu M, Akman F, Güneri A, Sarialioğlu F, Kargi A, et al. A rare tumor of craniofacial bones in children: a pediatric chondroblastic osteosarcoma case with diagnostic and therapeutic problems. Pediatr Hematol Oncol. 2001; 18:147–152.
Article18. Wittig JC, Bickels J, Priebat D, Jelinek J, Kellar-Graney K, Shmookler B, et al. Osteosarcoma: a multidisciplinary approach to diagnosis and treatment. Am Fam Physician. 2002; 65:1123–1132.19. Taran SJ, Taran R, Malipatil NB. Pediatric osteosarcoma: an updated review. Indian J Med Paediatr Oncol. 2017; 38:33–43.
Article20. Petrikowski CG, Pharoah MJ, Lee L, Grace MG. Radiographic differentiation of osteogenic sarcoma, osteomyelitis, and fibrous dysplasia of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80:744–750.
Article21. Dujardin F, Binh MB, Bouvier C, Gomez-Brouchet A, Larousserie F, Muret Ad, et al. MDM2 and CDK4 immunohistochemistry is a valuable tool in the differential diagnosis of low-grade osteosarcomas and other primary fibro-osseous lesions of the bone. Mod Pathol. 2011; 24:624–637.
Article22. Unni KK, Dahlin DC. Osteosarcoma: pathology and classification. Semin Roentgenol. 1989; 24:143–152.
Article23. Sanerkin NG. Definitions of osteosarcoma, chondrosarcoma, and fibrosarcoma of bone. Cancer. 1980; 46:178–185.
Article24. van den Berg H, Schreuder WH, de Lange J. Osteosarcoma: a comparison of jaw versus nonjaw localizations and review of the literature. Sarcoma. 2013; 2013:316123.
Article25. Costelloe CM, Chuang HH, Madewell JE. FDG PET/CT of primary bone tumors. AJR Am J Roentgenol. 2014; 202:W521–W531.
Article26. Hayden JB, Hoang BH. Osteosarcoma: basic science and clinical implications. Orthop Clin North Am. 2006; 37:1–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rosette-forming epithelioid osteosarcoma in the rib: a rare case of location and morphology
- Osteosarcoma arising on the surface of long bones: a review of radiologic and histologic spectrum in 9 cases
- Immunohistochemical Sdtudy of Cytokeratin and Epithelial Membrane Antigen Expression in Osteosarcoma
- Osteosarcoma of the mandible: A case report with an early radiographic manifestation
- Fibroblastic Type Osteosarcoma of the Ulna: a Case Report of a Tumor in a Rare Location with Atypical Imaging Findings
