Korean J Radiol.
2019 Sep;20(9):1334-1341. 10.3348/kjr.2019.0096.
Evaluation of Flow Pattern in the Ascending Aorta in Patients with Repaired Tetralogy of Fallot Using Four-Dimensional Flow Magnetic Resonance Imaging
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. dryj@yuhs.ac
- 2Division of Pediatric Cardiology, Severance Hospital, Department of Pediatrics, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Cardiovascular Surgery, Severance Cardiovascular Hospital, Department of Thoracic and Cardiovascular Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2455762
- DOI: http://doi.org/10.3348/kjr.2019.0096
Abstract
OBJECTIVE
To evaluate flow pattern characteristics in the ascending aorta (AA) with four-dimensional (4D)-flow MRI and to determine predictors of aortic dilatation late after tetralogy of Fallot (TOF) repair.
MATERIALS AND METHODS
This study included 44 patients with repaired TOF (25 males and 19 females; mean age, 28.9 ± 8.4 years) and 11 volunteers (10 males and 1 female, mean age, 33.7 ± 8.8 years) who had undergone 4D-flow MRI. The aortic diameters, velocity, wall shear stress (WSS), flow jet angle (FJA), and flow displacement (FD) at the level of the sinotubular junction (STJ) and mid-AA were compared between the repaired TOF and volunteer groups. The hemodynamic and clinical parameters were also compared between the aortic dilatation and non-dilatation subgroups in the repaired TOF group.
RESULTS
The diameters of the sinus of Valsalva, STJ, and AA were significantly higher in the repaired TOF group than in the volunteer group (p = 0.002, p < 0.001, and p = 0.013, respectively). The FJAs at the STJ and AA were significantly greater in the repaired TOF group (p < 0.001 and p = 0.003, respectively), while velocities and WSS parameters were significantly lower. FD showed no statistically significant difference (p = 0.817). In subgroup analysis, age at TOF repair was significantly higher (p = 0.039) and FJA at the level of the AA significantly greater (p = 0.003) and mean WSS were significantly lower (p = 0.039) in the aortic dilatation group. FD were higher in the aortic dilatation group without statistical significance (p = 0.217).
CONCLUSION
Patients with repaired TOF have an increased FJA, dilated AA, and secondarily decreased WSS. In addition to known risk factors, flow eccentricity may affect aortic dilatation in patients with repaired TOF.
Keyword
MeSH Terms
Figure
-
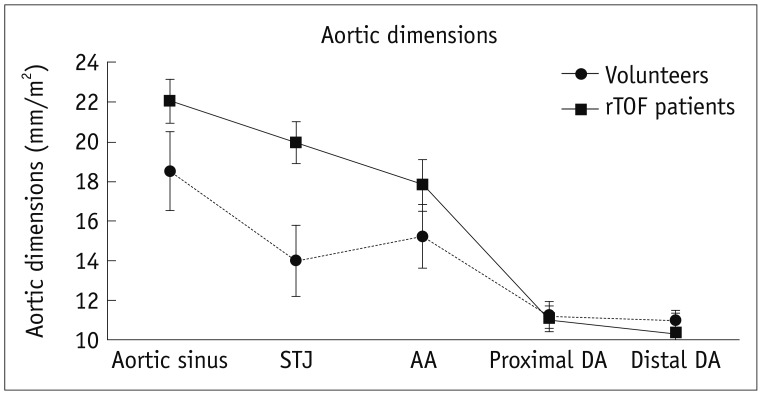
Fig. 1 Differences in aortic dimensions between patients with rTOF and healthy volunteers.AA = ascending aorta, DA = descending aorta, rTOF = repaired tetralogy of Fallot, STJ = sinotubular junction
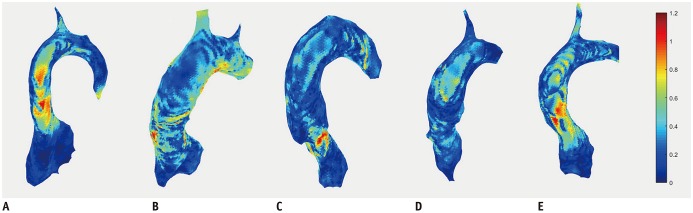
Fig. 2 Representative maximal WSS maps of volunteers and patients with rTOF.A. Volunteer. B. Aortic dilatation with high WSS group. C. Aortic dilatation with low WSS group. D. Non-aortic dilatation with low WSS group. E. Non-aortic dilatation with high WSS group. WSS = wall shear stress
Reference
-
1. Therrien J, Webb G. Clinical update on adults with congenital heart disease. Lancet. 2003; 362:1305–1313. PMID: 14575977.
Article2. Lillehei CW, Varco RL, Cohen M, Warden HE, Gott VL, DeWall RA, et al. The first open heart corrections of tetralogy of Fallot. A 26–31 year follow-up of 106 patients. Ann Surg. 1986; 204:490–502. PMID: 3767482.3. Niwa K, Siu SC, Webb GD, Gatzoulis MA. Progressive aortic root dilatation in adults late after repair of tetralogy of Fallot. Circulation. 2002; 106:1374–1378. PMID: 12221055.
Article4. Mongeon FP, Gurvitz MZ, Broberg CS, Aboulhosn J, Opotowsky AR, Kay JD, et al. Alliance for Adult Research in Congenital Cardiology (AARCC). Aortic root dilatation in adults with surgically repaired tetralogy of Fallot: a multicenter cross-sectional study. Circulation. 2013; 127:172–179. PMID: 23224208.5. Dodds GA 3rd, Warnes CA, Danielson GK. Aortic valve replacement after repair of pulmonary atresia and ventricular septal defect or tetralogy of Fallot. J Thorac Cardiovasc Surg. 1997; 113:736–741. PMID: 9104983.
Article6. Capelli H, Ross D, Somerville J. Aortic regurgitation in tetrad of Fallot and pulmonary atresia. Am J Cardiol. 1982; 49:1979–1983. PMID: 7081079.
Article7. Ordovas KG, Keedy A, Naeger DM, Kallianos K, Foster E, Liu J, et al. Dilatation of the ascending aorta is associated with presence of aortic regurgitation in patients after repair of tetralogy of Fallot. Int J Cardiovasc Imaging. 2016; 32:1265–1272. PMID: 27240599.
Article8. Rathi VK, Doyle M, Williams RB, Yamrozik J, Shannon RP, Biederman RW. Massive aortic aneurysm and dissection in repaired tetralogy of Fallot; diagnosis by cardiovascular magnetic resonance imaging. Int J Cardiol. 2005; 101:169–170. PMID: 15860407.
Article9. Kim WH, Seo JW, Kim SJ, Song J, Lee J, Na CY. Aortic dissection late after repair of tetralogy of Fallot. Int J Cardiol. 2005; 101:515–516. PMID: 15907429.
Article10. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. J Magn Reson Imaging. 2012; 36:1015–1036. PMID: 23090914.
Article11. Sievers HH, Putman LM, Kheradvar A, Gabbert D, Wegner P, Scheewe J, et al. 4D flow streamline characteristics of the great arteries twenty years after Lecompte and direct spiral arterial switch operation (DSASO) in simple TGA. Glob Cardiol Sci Pract. 2016; 2016:e201629. PMID: 29043274.
Article12. Meierhofer C, Schneider EP, Lyko C, Hutter A, Martinoff S, Markl M, et al. Wall shear stress and flow patterns in the ascending aorta in patients with bicuspid aortic valves differ significantly from tricuspid aortic valves: a prospective study. Eur Heart J Cardiovasc Imaging. 2013; 14:797–804. PMID: 23230276.
Article13. Rodríguez-Palomares JF, Dux-Santoy L, Guala A, Kale R, Maldonado G, Teixidó-Turà G, et al. Aortic flow patterns and wall shear stress maps by 4D-flow cardiovascular magnetic resonance in the assessment of aortic dilatation in bicuspid aortic valve disease. J Cardiovasc Magn Reson. 2018; 20:28. PMID: 29695249.
Article14. Piatti F, Sturla F, Bissell MM, Pirola S, Lombardi M, Nesteruk I, et al. 4D flow analysis of BAV-related fluid-dynamic alterations: evidences of wall shear stress alterations in absence of clinically-relevant aortic anatomical remodeling. Front Physiol. 2017; 8:441. PMID: 28694784.
Article15. Fong Y, Di C, Huang Y, Gilbert PB. Model-robust inference for continuous threshold regression models. Biometrics. 2017; 73:452–462. PMID: 27858965.
Article16. Gräfe D, Gutberlet M, Mende M, Dähnert I, Lücke C, Kostelka M, et al. Cross-sectional areas of the thoracic aorta in children and adolescents with repaired tetralogy of Fallot obtained by cardiac magnetic resonance angiography. J Thorac Imaging. 2018; 33:105–111. PMID: 29232281.
Article17. Niwa K. Aortic root dilatation in tetralogy of Fallot long-term after repair--histology of the aorta in tetralogy of Fallot: evidence of intrinsic aortopathy. Int J Cardiol. 2005; 103:117–119. PMID: 16080967.
Article18. Bonello B, Shore DF, Uebing A, Diller GP, Keegan J, Burman ED, et al. Aortic dilatation in repaired tetralogy of Fallot. JACC Cardiovasc Imaging. 2018; 11:150–152. PMID: 28412425.
Article19. Nagy CD, Alejo DE, Corretti MC, Ravekes WJ, Crosson JE, Spevak PJ, et al. Tetralogy of Fallot and aortic root dilation: a long-term outlook. Pediatr Cardiol. 2013; 34:809–816. PMID: 23080541.
Article20. Bieging ET, Frydrychowicz A, Wentland A, Landgraf BR, Johnson KM, Wieben O, et al. In vivo three-dimensional MR wall shear stress estimation in ascending aortic dilatation. J Magn Reson Imaging. 2011; 33:589–597. PMID: 21563242.
Article21. Barker AJ, Markl M, Bürk J, Lorenz R, Bock J, Bauer S, et al. Bicuspid aortic valve is associated with altered wall shear stress in the ascending aorta. Circ Cardiovasc Imaging. 2012; 5:457–466. PMID: 22730420.
Article22. Geiger J, Hirtler D, Gottfried K, Rahman O, Bollache E, Barker AJ, et al. Longitudinal evaluation of aortic hemodynamics in Marfan syndrome: new insights from a 4D flow cardiovascular magnetic resonance multi-year follow-up study. J Cardiovasc Magn Reson. 2017; 19:33. PMID: 28327193.
Article23. Farag ES, van Ooij P, Planken RN, Dukker KCP, de Heer F, Bouma BJ, et al. Aortic valve stenosis and aortic diameters determine the extent of increased wall shear stress in bicuspid aortic valve disease. J Magn Reson Imaging. 2018; 48:522–530. PMID: 29451963.
Article24. van Ooij P, Markl M, Collins JD, Carr JC, Rigsby C, Bonow RO, et al. Aortic valve stenosis alters expression of regional aortic wall shear stress: new insights from a 4-dimensional flow magnetic resonance imaging study of 571 subjects. J Am Heart Assoc. 2017; 6:pii: e005959.
Article25. Dyverfeldt P, Bissell M, Barker AJ, Bolger AF, Carlhäll CJ, Ebbers T, et al. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson. 2015; 17:72. PMID: 26257141.
Article26. Sigovan M, Hope MD, Dyverfeldt P, Saloner D. Comparison of four-dimensional flow parameters for quantification of flow eccentricity in the ascending aorta. J Magn Reson Imaging. 2011; 34:1226–1230. PMID: 21928387.
Article27. Garcia J, Barker AJ, Murphy I, Jarvis K, Schnell S, Collins JD, et al. Four-dimensional flow magnetic resonance imaging-based characterization of aortic morphometry and haemodynamics: impact of age, aortic diameter, and valve morphology. Eur Heart J Cardiovasc Imaging. 2016; 17:877–884. PMID: 26377908.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aortic Root and Ascending Aortic Aneurysm in an Adult with a Repaired Tetralogy of Fallot
- Demonstration of Turbulence at the Site of Ascending Aorta Graft Kinking Using 4-Dimensional Flow Magnetic Resonance Imaging
- Echocardiographic Findings in Tetralogy of Fallot
- Semiautomatic Three-Dimensional Threshold-Based Cardiac Computed Tomography Ventricular Volumetry in Repaired Tetralogy of Fallot: Comparison with Cardiac Magnetic Resonance Imaging
- Four-Dimensional Flow Magnetic Resonance Imaging for Cardiovascular Imaging: from Basic Concept to Clinical Application
