Duration of Treatment Effect of Extracorporeal Shock Wave on Spasticity and Subgroup-Analysis According to Number of Shocks and Application Site: A Meta-Analysis
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Seoul Medical Center, Seoul, Korea. rehabdoc@seoulmc.or.kr
- KMID: 2448999
- DOI: http://doi.org/10.5535/arm.2019.43.2.163
Abstract
OBJECTIVE
To investigate duration of the treatment effect of extracorporeal shockwave therapy (ESWT) on spasticity levels measured with Modified Ashworth Scale (MAS) regardless of the patient group (stroke, multiple sclerosis, and cerebral palsy) and evaluate its spasticity-reducing effect depending on the number of shocks and site of application.
METHODS
PubMed, EMBASE, the Cochrane Library, and Scopus were searched from database inception to February 2018. Randomized controlled trials and cross-over trials were included. All participants had spasticity regardless of cause. ESWT was the main intervention and MAS score was the primary outcome. Among 122 screened articles, 9 trials met the inclusion criteria.
RESULTS
The estimate of effect size showed statistically significant MAS grade reduction immediately after treatment (standardized mean difference [SMD]=-0.57; 95% confidence interval [CI], -1.00 to -0.13; p=0.012), 1 week after (SMD=-1.81; 95% CI, -3.07 to -0.55; p=0.005), 4 weeks after (SMD=-2.35; 95% CI, -3.66 to -1.05; p<0.001), and 12 weeks after (SMD=-1.07; 95% CI, -2.04 to -0.10; p=0.03). Meta-regression and subgroup analysis were performed for the "˜immediately after ESWT application' group. The prediction equation obtained from metaregression was -1.0824+0.0002* (number of shocks), which was not statistically significant. Difference in MAS grade reduction depending on site of application was not statistically significant either in subgroup analysis (knee and ankle joints vs. elbow, wrist, and finger joints).
CONCLUSION
ESWT effectively reduced spasticity levels measured with MAS regardless of patient group. Its effect maintained for 12 weeks. The number of shocks or site of application had no significant influence on the therapeutic effect of ESWT in reducing spasticity. Ongoing trials with ESWT are needed to address optimal parameters of shock wave to reduce spasticity regarding intensity, frequency, and numbers.
MeSH Terms
Figure
-

Fig. 1. Preferred Reporting Items for Systemic Reviews and MetaAnalysis (PRISMA) flow chart. RCT, randomized controlled trial; ES, electrical stimulation; ESWT, extracorporeal shockwave therapy; MAS, Modified Ashworth Scale.
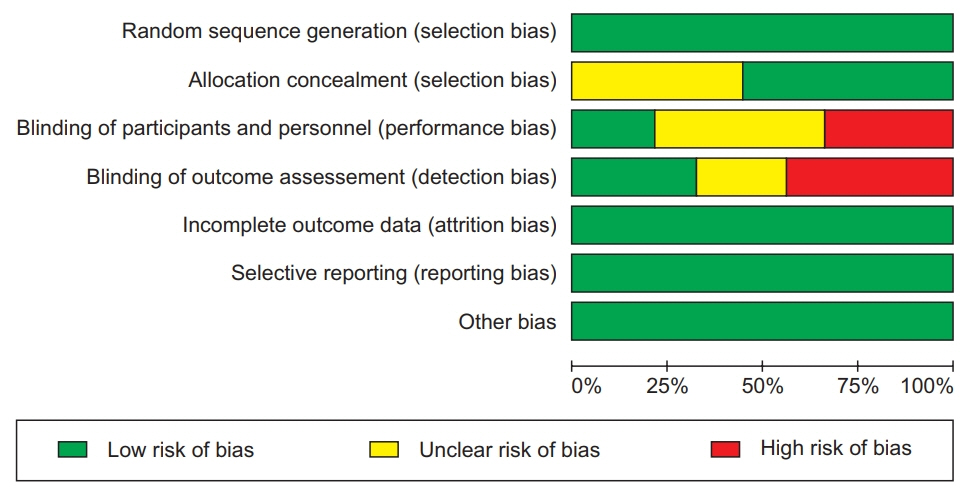
Fig. 2. Risk of bias graph illustrating the proportion of studies with each judgement (‘Yes’, ‘No’, or ‘Unclear’) for each entry in the tool.

Fig. 3. Risk of bias summary. It presented all judgements in a cross-tabulation of study by entry of + (Yes), – (No), and ? (Unclear).
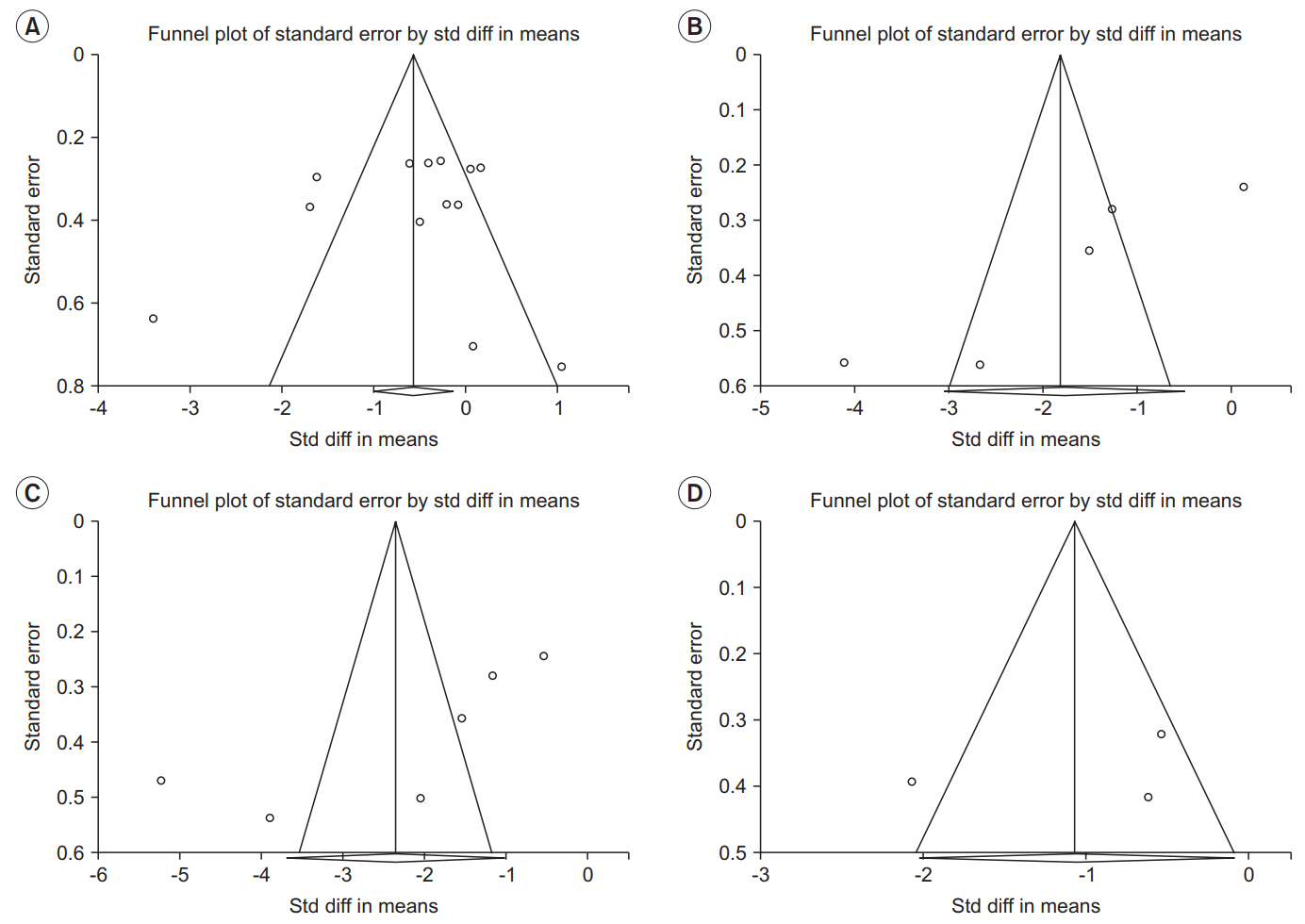
Fig. 4. Funnel plot to evaluate publication bias at (A) immediately after ESWT application, (B) 1 week after ESWT application, (C) 4 weeks after ESWT application, and (D) 12 weeks after ESWT application. Std diff, standard difference. ESWT, extracorporeal shockwave therapy.
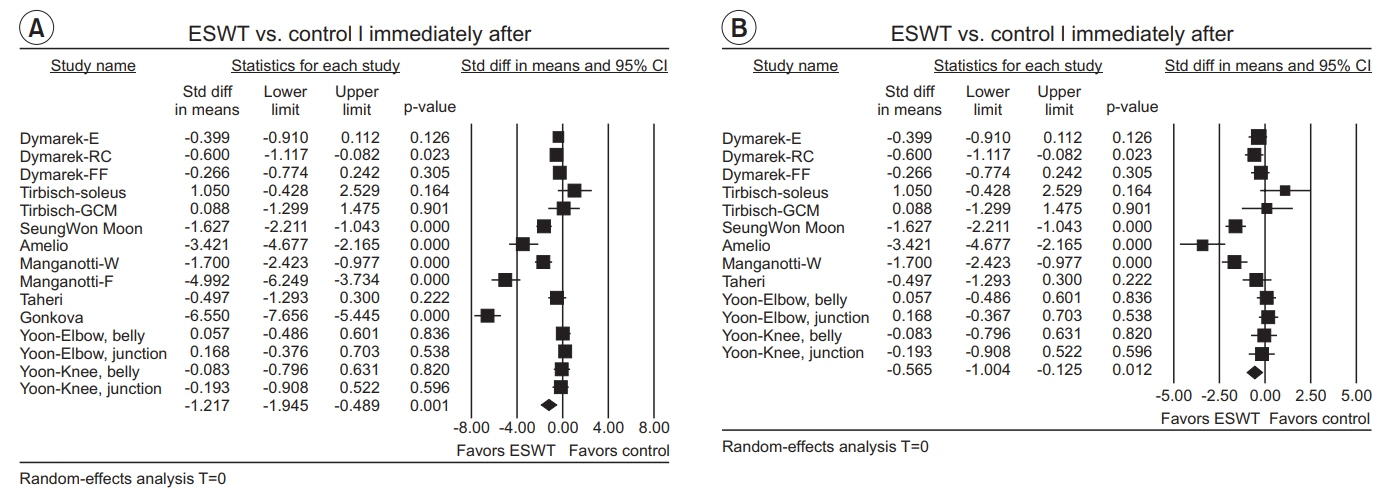
Fig. 5. Forest plot of effect sizes at (A) immediately after ESWT application, (B) after excluding outliers (Manganotti-F and Gonkova). ESWT, extracorporeal shockwave therapy; Std diff, standard difference; CI, confidence interval; E, elbow joint; RC, radio-carpal joint; FF, finger joints; GCM, gastrocnemius; W, wrist flexors; F, finger flexors.
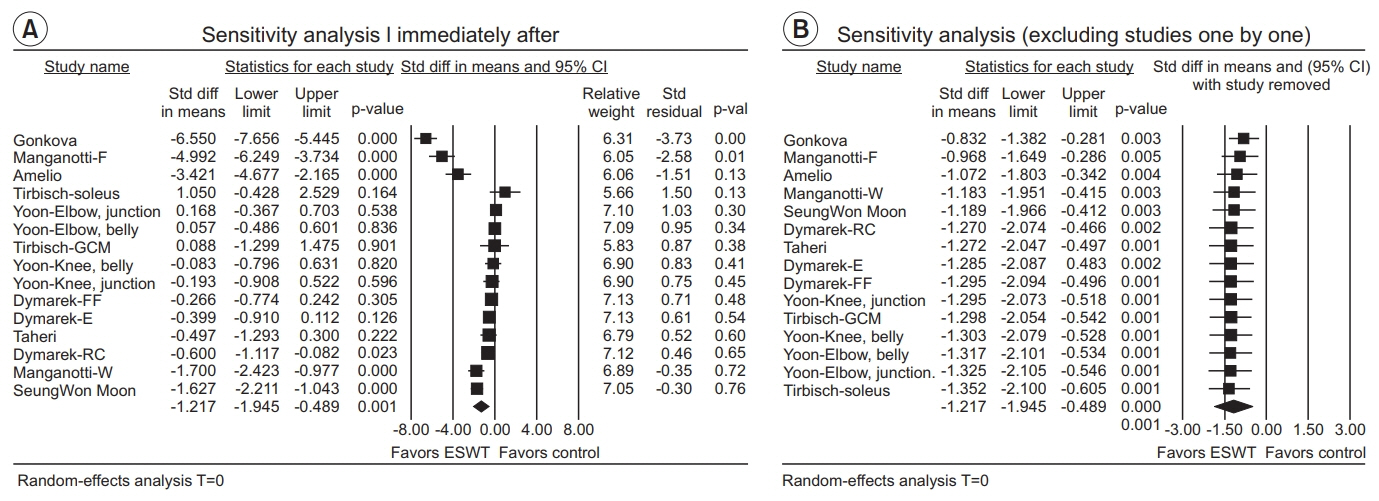
Fig. 6. (A) Sensitivity analysis with effect sizes, sample size, weight, and residual (immediately after ESWT application). (B) Sensitivity analysis with effect sizes after excluding studies one by one (immediately after ESWT application). ESWT, extracorporeal shockwave therapy; Std diff, standard difference; CI, confidence interval; E, elbow joint; RC, radio-carpal joint; FF, finger joints; GCM, gastrocnemius; W, wrist flexors; F, finger flexors.

Fig. 7. (A) Sensitivity analysis with effect sizes, sample size, weight, and residual (1 week after ESWT application). (B) Sensitivity analysis with effect sizes after excluding studies one by one (1 week after ESWT application). ESWT, extracorporeal shockwave therapy; Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.
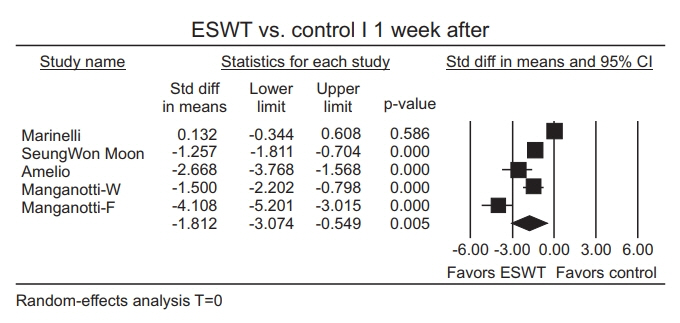
Fig. 8. Forest plot of the effect sizes 1 week after extracorporeal shockwave therapy (ESWT). Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.

Fig. 9. (A) Sensitivity analysis with effect sizes, sample size, weight, and residual (4 weeks after the ESWT application). (B) Sensitivity analysis with effect sizes after excluding studies one by one (4 weeks after the ESWT application). ESWT, extracorporeal shockwave therapy; Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.
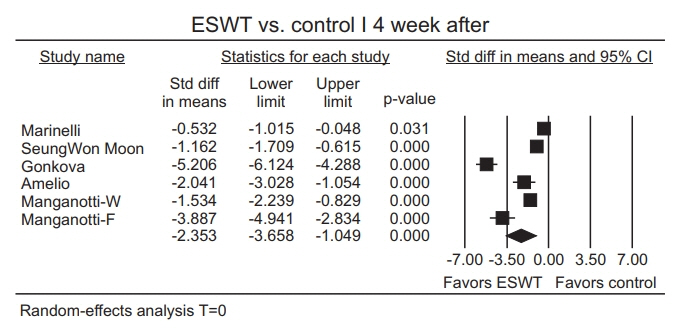
Fig. 10. Forest plot of effect sizes 4 weeks after extracorporeal shockwave therapy (ESWT). Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.
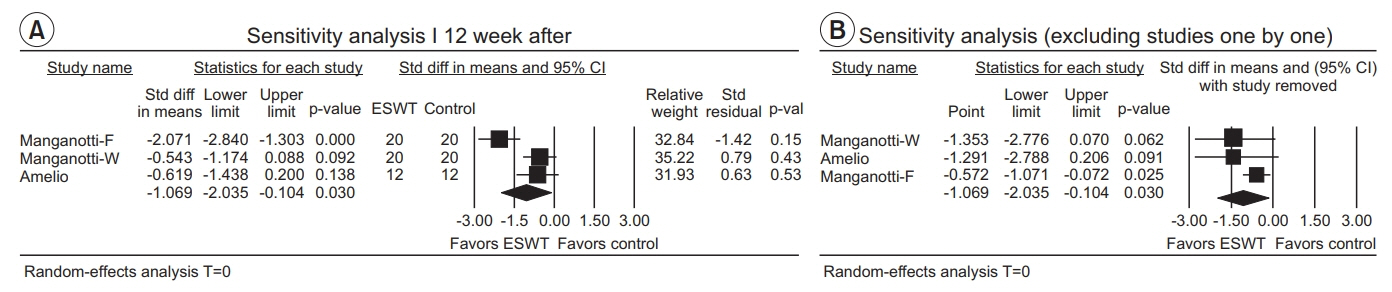
Fig. 11. (A) Sensitivity analysis with effect sizes, sample size, weight, and residual (12 weeks after ESWT application). (B) Sensitivity analysis with effect sizes after excluding studies one by one (12 weeks after ESWT application). ESWT, extracorporeal shockwave therapy; Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.

Fig. 12. Forest plot of the effect sizes 12 weeks after extracorporeal shockwave therapy (ESWT). Std diff, standard difference; CI, confidence interval; W, wrist flexors; F, finger flexors.
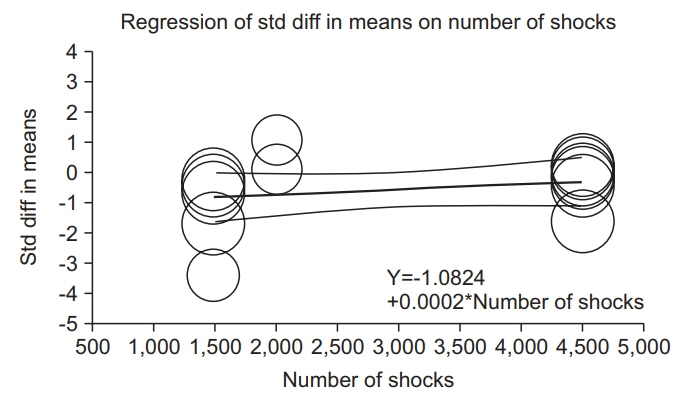
Fig. 13. Scatterplot of meta-regression under the randomeffects model (immediately after ESWT application). ESWT, extracorporeal shockwave therapy.

Fig. 14. Forest plots of knee and ankle-joints group and elbow, wrist, and finger joints group depending on the application site (immediately after ESWT application). ESWT, extracorporeal shockwave therapy; E, elbow joint; RC, radio-carpal joint; FF, finger joints; GCM, gastrocnemius.
Reference
-
1. Lance JW. Symposium synopsis. In : Feldman RG, Young RR, Koella WP, editors. Spasticity: disordered motor control. Chicago: Year Book Medical Publishers;1980. p. 485–4.2. Sheean G. The pathophysiology of spasticity. Eur J Neurol. 2002; 9 Suppl 1:3–9.
Article3. Tsai KH, Yeh CY, Chang HY, Chen JJ. Effects of a single session of prolonged muscle stretch on spastic muscle of stroke patients. Proc Natl Sci Counc Repub China B. 2001; 25:76–81.4. Matsumoto S, Kawahira K, Etoh S, Ikeda S, Tanaka N. Short-term effects of thermotherapy for spasticity on tibial nerve F-waves in post-stroke patients. Int J Biometeorol. 2006; 50:243–50.
Article5. Levin MF, Hui-Chan C. Are H and stretch reflexes in hemiparesis reproducible and correlated with spasticity? J Neurol. 1993; 240:63–71.
Article6. Panizza M, Balbi P, Russo G, Nilsson J. H-reflex recovery curve and reciprocal inhibition of H-reflex of the upper limbs in patients with spasticity secondary to stroke. Am J Phys Med Rehabil. 1995; 74:357–63.
Article7. Morris S. Ashworth and Tardieu Scales: their clinical relevance for measuring spasticity in adult and paediatric neurological populations. Phys Ther Rev. 2002; 7:53–62.
Article8. Yan T, Hui-Chan CW, Li LS. Functional electrical stimulation improves motor recovery of the lower extremity and walking ability of subjects with first acute stroke: a randomized placebo-controlled trial. Stroke. 2005; 36:80–5.9. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987; 67:206–7.
Article10. Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 1980; 2:1265–8.
Article11. Wang CJ. Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res. 2012; 7:11.
Article12. Manganotti P, Amelio E. Long-term effect of shock wave therapy on upper limb hypertonia in patients affected by stroke. Stroke. 2005; 36:1967–71.
Article13. Dymarek R, Taradaj J, Rosinczuk J. The effect of radial extracorporeal shock wave stimulation on upper limb spasticity in chronic stroke patients: a single-blind, randomized, placebo-controlled study. Ultrasound Med Biol. 2016; 42:1862–75.
Article14. Gonkova MI, Ilieva EM, Ferriero G, Chavdarov I. Effect of radial shock wave therapy on muscle spasticity in children with cerebral palsy. Int J Rehabil Res. 2013; 36:284–90.
Article15. Amelio E, Manganotti P. Effect of shock wave stimulation on hypertonic plantar flexor muscles in patients with cerebral palsy: a placebo-controlled study. J Rehabil Med. 2010; 42:339–43.
Article16. Marinelli L, Mori L, Solaro C, Uccelli A, Pelosin E, Curra A, et al. Effect of radial shock wave therapy on pain and muscle hypertonia: a double-blind study in patients with multiple sclerosis. Mult Scler. 2015; 21:622–9.
Article17. Lee JY, Kim SN, Lee IS, Jung H, Lee KS, Koh SE. Effects of extracorporeal shock wave therapy on spasticity in patients after brain injury: a meta-analysis. J Phys Ther Sci. 2014; 26:1641–7.18. Guo P, Gao F, Zhao T, Sun W, Wang B, Li Z. Positive effects of extracorporeal shock wave therapy on spasticity in poststroke patients: a meta-analysis. J Stroke Cerebrovasc Dis. 2017; 26:2470–2476.
Article19. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009; 62:1006–12.
Article20. Higgins J, Deeks JJ, Altman DG. Special topics in statistics. In : Higgins J, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons;2008. p. 481–530.21. Higgins J, Altman DG. Assessing risk of bias in included studies. In : Higgins J, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons;2008. p. 184–242.22. Deeks JJ, Higgins J, Altman DG. Analysing data and undertaking meta-analyses. In : Higgins J, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons;2008. p. 243–96.23. Taheri P, Vahdatpour B, Mellat M, Ashtari F, Akbari M. Effect of extracorporeal shock wave therapy on lower limb spasticity in stroke patients. Arch Iran Med. 2017; 20:338–43.24. Yoon SH, Shin MK, Choi EJ, Kang HJ. Effective site for the application of extracorporeal shock-wave therapy on spasticity in chronic stroke: muscle belly or myotendinous junction. Ann Rehabil Med. 2017; 41:547–55.
Article25. Tirbisch L. Effects of radial shock wave therapy on sural triceps spasticity in hemiplegic patients in subacute phase: a controlled randomized trial. Kinésithérapie. 2015; 15:62–9.26. Moon SW, Kim JH, Jung MJ, Son S, Lee JH, Shin H, et al. The effect of extracorporeal shock wave therapy on lower limb spasticity in subacute stroke patients. Ann Rehabil Med. 2013; 37:461–70.
Article27. Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Stat Med. 2007; 26:4544–62.
Article28. Santamato A, Micello MF, Panza F, Fortunato F, Logroscino G, Picelli A, et al. Extracorporeal shock wave therapy for the treatment of poststroke plantar-flexor muscles spasticity: a prospective open-label study. Top Stroke Rehabil. 2014; 21 Suppl 1:S17–24.
Article29. Kim YW, Shin JC, Yoon JG, Kim YK, Lee SC. Usefulness of radial extracorporeal shock wave therapy for the spasticity of the subscapularis in patients with stroke: a pilot study. Chin Med J (Engl). 2013; 126:4638–43.30. Sohn MK, Cho KH, Kim YJ, Hwang SL. Spasticity and electrophysiologic changes after extracorporeal shock wave therapy on gastrocnemius. Ann Rehabil Med. 2011; 35:599–604.
Article31. Kim JH, Kim JY, Choi CM, Lee JK, Kee HS, Jung KI, Yoon SR. The dose-related effects of extracorporeal shock wave therapy for knee osteoarthritis. Ann Rehabil Med. 2015; 39:616–23.
Article32. Zhang X, Yan X, Wang C, Tang T, Chai Y. The doseeffect relationship in extracorporeal shock wave therapy: the optimal parameter for extracorporeal shock wave therapy. J Surg Res. 2014; 186:484–92.
Article33. Wang CJ, Yang KD, Wang FS, Hsu CC, Chen HH. Shock wave treatment shows dose-dependent enhancement of bone mass and bone strength after fracture of the femur. Bone. 2004; 34:225–30.
Article34. Rompe JD, Kirkpatrick CJ, Kullmer K, Schwitalle M, Krischek O. Dose-related effects of shock waves on rabbit tendo Achillis: a sonographic and histological study. J Bone Joint Surg Br. 1998; 80:546–52.35. Sehgal N, McGuire JR. Beyond Ashworth: electrophysiologic quantification of spasticity. Phys Med Rehabil Clin N Am. 1998; 9:949–79.
Article36. Eisen A, Odusote K. Amplitude of the F wave: a potential means of documenting spasticity. Neurology. 1979; 29(9 Pt 1):1306–9.
Article37. Hultborn H, Nielsen JB. H‐reflexes and F‐responses are not equally sensitive to changes in motoneuronal excitability. Muscle Nerve. 1995; 18:1471–4.
Article38. Bakheit AM, Maynard VA, Curnow J, Hudson N, Kodapala S. The relation between Ashworth scale scores and the excitability of the alpha motor neurones in patients with post-stroke muscle spasticity. J Neurol Neurosurg Psychiatry. 2003; 74:646–8.
Article39. Dymarek R, Ptaszkowski K, Słupska L, Halski T, Taradaj J, Rosinczuk J. Effects of extracorporeal shock wave on upper and lower limb spasticity in poststroke patients: a narrative review. Top Stroke Rehabil. 2016; 23:293–303.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Extracorporeal Shock Wave Lithortripsy Experimentally Induced Cholelithiasis and Organs in the Dog
- Spasticity and Electrophysiologic Changes after Extracorporeal Shock Wave Therapy on Gastrocnemius
- Extracorporeal Shock Wave Therapy and Quantitative Ultrasonographic Evaluation of the Rheologic Effect in the Patients with Post-stroke Upper Limb Spasticity: A Case Report
- Current Concepts in Extracorporeal Shock Wave Therapy
- Effective Site for the Application of Extracorporeal Shock-Wave Therapy on Spasticity in Chronic Stroke: Muscle Belly or Myotendinous Junction
