Quilty Lesions in the Endomyocardial Biopsies after Heart Transplantation
- Affiliations
-
- 1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jsunkim@skku.edu
- 2Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Health Sciences and Technology, Sungkyunkwan University, SAIHST, Seoul, Korea.
- KMID: 2437578
- DOI: http://doi.org/10.4132/jptm.2018.11.30
Abstract
- BACKGROUND
The aim of this study was to investigate the clinical significance of Quilty lesions in endomyocardial biopsies (EMBs) of cardiac transplantation patients.
METHODS
A total of 1190 EMBs from 117 cardiac transplantation patients were evaluated histologically for Quilty lesions, acute cellular rejection, and antibody-mediated rejection. Cardiac allograft vasculopathy was diagnosed by computed tomography coronary angiography. Clinical information, including the patients' survival was retrieved by a review of medical records.
RESULTS
Eighty-eight patients (75.2%) were diagnosed with Quilty lesions, which were significantly associated with acute cellular rejection, but not with acute cellular rejection ≥ 2R or antibody-mediated rejection. In patient sdiagnosed with both Quilty lesions and acute cellular rejection, the time-to-onset of Quilty lesions from transplantation was longer than that of acute cellular rejections. We found a significant association between Quilty lesions and cardiac allograft vasculopathy. No significant relationship was found between Quilty lesions and the patients' survival.
CONCLUSIONS
Quilty lesion may be an indicator of previous acute cellular rejection rather than a predictor for future acute cellular rejection.
Keyword
Figure
-
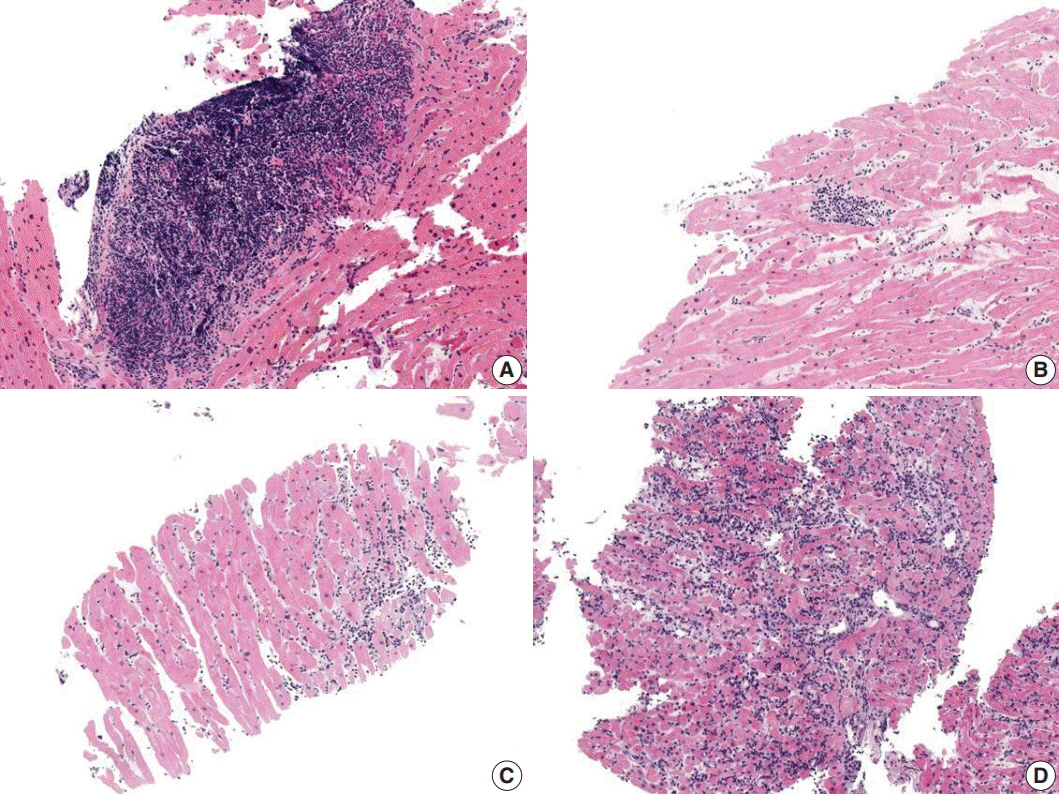
Fig. 1. Quilty lesion and acute cellular rejection. (A) Quilty lesion. (B) Grade 1R. (C) Grade 2R. (D) Grade 3R.

Fig. 2. Antibody-mediated rejection. (A) Swollen endothelial cells and intravascular mononuclear cells. (B) Multifocal C4d staining in capillary endothelial cells. (C) CD 68 staining in intravascular macrophages (arrow).

Fig. 3. Then number of Quilty-positive endomyocardial biopsies (EMBs) for each biopsy order. The number of Quilty-positive EMBs increases as biopsy order increases.

Fig. 4. Time-to-onset from cardiac transplantation to acute cellular rejection (ACR) and Quilty lesions. The time-to-onset of Quilty lesion is significantly longer than that of acute cellular rejection.
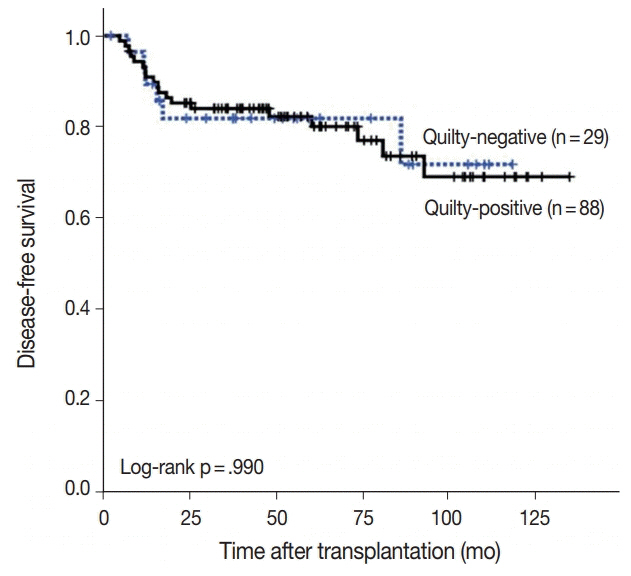
Fig. 5. Kaplan-Meier analysis for disease-free survival (death, graft loss) in Quilty-positive and Quilty-negative patients. The difference in survival between Quilty-positive and Quilty-negative is not significant.
Reference
-
1. Lund LH, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirtieth official adult heart transplant report 2013: focus theme: age. J Heart Lung Transplant. 2013; 32:951–64.2. Joshi A, Masek MA, Brown BW Jr, Weiss LM, Billingham ME. “Quilty” revisited: a 10-year perspective. Hum Pathol. 1995; 26:547–57.
Article3. Marboe CC, Billingham M, Eisen H, et al. Nodular endocardial infiltrates (Quilty lesions) cause significant variability in diagnosis of ISHLT Grade 2 and 3A rejection in cardiac allograft recipients. J Heart Lung Transplant. 2005; 24(7 Suppl):S219–26.
Article4. Mozaffari K, Bakhshandeh H, Amin A, et al. Diagnostic pitfalls and challenges in interpretation of heart transplantation rejection in endomyocardial biopsies with focus on our experience. Res Cardiovasc Med. 2014; 3:e13986.
Article5. Stewart S, Winters GL, Fishbein MC, et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant. 2005; 24:1710–20.
Article6. Kottke-Marchant K, Ratliff NB. Endomyocardial lymphocytic infiltrates in cardiac transplant recipients: incidence and characterization. Arch Pathol Lab Med. 1989; 113:690–8.7. Radio SJ, McManus BM, Winters GL, et al. Preferential endocardial residence of B-cells in the “Quilty effect” of human heart allografts: immunohistochemical distinction from rejection. Mod Pathol. 1991; 4:654–60.8. Chu KE, Ho EK, de la Torre L, Vasilescu ER, Marboe CC. The relationship of nodular endocardial infiltrates (Quilty lesions) to survival, patient age, anti-HLA antibodies, and coronary artery disease following heart transplantation. Cardiovasc Pathol. 2005; 14:219–24.
Article9. Costanzo-Nordin MR, Winters GL, Fisher SG, et al. Endocardial infiltrates in the transplanted heart: clinical significance emerging from the analysis of 5026 endomyocardial biopsy specimens. J Heart Lung Transplant. 1993; 12:741–7.10. Pardo-Mindan FJ, Lozano MD. "Quilty effect" in heart transplantation: is it related to acute rejection? J Heart Lung Transplant. 1991; 10:937–41.11. Smith RN, Chang Y, Houser S, Dec GW, Grazette L. Higher frequency of high-grade rejections in cardiac allograft patients after Quilty B lesions or grade 2/4 rejections. Transplantation. 2002; 73:1928–32.
Article12. Zakliczynski M, Nozynski J, Konecka-Mrowka D, et al. Quilty effect correlates with biopsy-proven acute cellular rejection but does not predict transplanted heart coronary artery vasculopathy. J Heart Lung Transplant. 2009; 28:255–9.
Article13. Suit PF, Kottke-Marchant K, Ratliff NB, Pippenger CE, Easely K. Comparison of whole-blood cyclosporine levels and the frequency of endomyocardial lymphocytic infiltrates (the Quilty lesion) in cardiac transplantation. Transplantation. 1989; 48:618–21.14. Colvin-Adams M, Agnihotri A. Cardiac allograft vasculopathy: current knowledge and future direction. Clin Transplant. 2011; 25:175–84.
Article15. Hosenpud JD, Shipley GD, Wagner CR. Cardiac allograft vasculopathy: current concepts, recent developments, and future directions. J Heart Lung Transplant. 1992; 11(1 Pt 1):9–23.16. Hiemann NE, Knosalla C, Wellnhofer E, Lehmkuhl HB, Hetzer R, Meyer R. Quilty indicates increased risk for microvasculopathy and poor survival after heart transplantation. J Heart Lung Transplant. 2008; 27:289–96.
Article17. Yamani MH, Ratliff NB, Starling RC, et al. Quilty lesions are associated with increased expression of vitronectin receptor (alphavbeta3) and subsequent development of coronary vasculopathy. J Heart Lung Transplant. 2003; 22:687–90.18. Szymanska S, Grajkowska W, Sobieszczanska-Malek M, Zielinski T, Pyzlak M, Pronicki M. Prevalence of the Quilty effect in endomyocardial biopsy of patients after heart transplantation: from cellular rejection to antibody-mediated rejection? Pol J Pathol. 2016; 67:216–20.19. Cano LC, Arteta AA, Fernández R, et al. Quilty effect areas are frequently associated with endocardial C4d deposition. J Heart Lung Transplant. 2008; 27:775–9.
Article20. Hiemann NE, Knosalla C, Wellnhofer E, Lehmkuhl HB, Hetzer R, Meyer R. Quilty in biopsy is associated with poor prognosis after heart transplantation. Transpl Immunol. 2008; 19:209–14.
Article21. Chambers DC, Yusen RD, Cherikh WS, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Lung And Heart-Lung Transplantation Report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant. 2017; 36:1047–59.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pathologic Analysis of Endomyocardial Biopsies in Heart Transplantation
- Pathological Analysis of Post-Transplantation Endomyocardial Biopsies
- Recent Advancement in Heart and Lung Transplantation
- Heart Transplantation Performed in a Patient with Isolated Cardiac Sarcoidosis
- Current Status of Heart Transplantation and Left Ventricular Assist Device: Major Changes in the Last Decade
